Introduction
-
Ankle injuries are among the most common lower limb injuries, ranging from simple sprains to complex fractures.
-
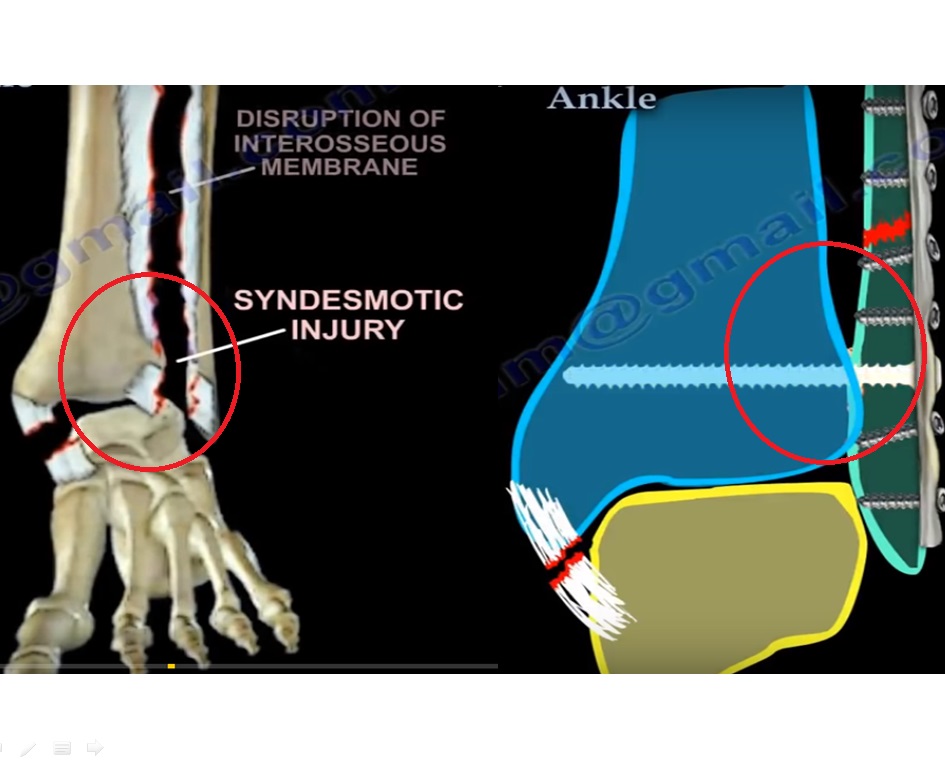
The distal tibiofibular syndesmosis is essential for ankle stability and consists of:
-
Anterior inferior tibiofibular ligament
-
Posterior inferior tibiofibular ligament
-
Interosseous ligament
-
Interosseous membrane
-
-
Acute ankle diastasis injury refers to disruption of the distal tibiofibular syndesmosis, either as:
-
An isolated ligamentous injury, or
-
An injury associated with malleolar fractures
-
-
Approximately 65.8 percent of ankle fractures are associated with acute syndesmotic injury.
Consequences of Inadequate Treatment
Untreated or poorly reduced syndesmosis injuries can result in:
-
Chronic ankle pain
-
Post-traumatic osteoarthritis
-
Persistent ankle instability
-
Poor long-term functional outcomes
Clinical Significance
-
Given the high incidence and morbidity of these injuries, a clinically effective and cost-efficient treatment strategy is essential.
-
There is no universal consensus regarding:
-
Optimal diagnostic methods
-
Implant selection
-
Surgical technique
-
Postoperative rehabilitation protocols
-
Treatment Modalities
Three primary treatment strategies are used for acute ankle diastasis injuries:
Static Fixation
-
Utilizes syndesmosis screws:
-
One or two tricortical or quadricortical screws
-
Screw diameter ranges from 3.5 to 6.0 millimeters
-
-
Widely used traditional method
-
Common complications include:
-
Screw breakage
-
Need for routine implant removal
-
Increased reoperation rates
-
Dynamic Fixation
-
Uses a suture button device consisting of:
-
Two metallic buttons
-
A high-strength connecting suture
-
-
Provides elastic fixation
-
Allows physiologic micromotion of the syndesmosis
Anatomic Ligament Repair
-
Involves direct repair of the anterior inferior tibiofibular ligament using a suture anchor
-
Syndesmosis reduction performed under direct visualization
-
Reduction confirmed with intraoperative imaging
Management of Combined Injuries and Rationale for Review
-
In ankle fractures involving syndesmotic injury:
-
Malleolar fractures are stabilized first, usually with plate fixation
-
Disrupted syndesmotic ligaments are then repaired anatomically
-
Additional fixation is added if reduction remains unstable
-
-
Ongoing controversy exists regarding the most effective treatment method.
-
Previous studies typically compare only two techniques.
-
The purpose of this analysis was to compare:
-
Static fixation
-
Dynamic fixation
-
Anatomic repair
-
-
The goal was to identify the most effective and reliable treatment strategy for acute ankle diastasis injuries.
Methods
-
A systematic review and meta-analysis methodology was used.
-
Literature searches were conducted using major medical databases.
-
Search terms focused on syndesmosis fixation techniques and anatomic ligament repair.
Study Selection Criteria
Included Studies
-
Randomized controlled trials
-
Prospective cohort studies
-
Retrospective cohort studies
Required Comparisons
-
At least two treatment methods, such as:
-
Dynamic versus static fixation
-
Static fixation versus anatomic repair
-
Required Outcomes
-
American Orthopaedic Foot and Ankle Society score
-
Visual Analog Scale pain score
-
Implant failure or irritation
-
Infection rates
-
Reoperation rates
Excluded Studies
-
Meta-analyses and systematic reviews
-
Studies without defined outcome measures
-
Studies with unclear or poorly defined comparison groups
Data Compilation Strategy
-
No direct comparative studies between dynamic fixation and anatomic repair were identified.
-
To address this limitation:
-
Data from studies using dynamic fixation were pooled
-
Data from studies using anatomic repair were pooled
-
-
Outcomes analyzed included:
-
Functional scores at 1 year
-
Pain scores at 1 year
-
Reoperation rates
-
Quality Assessment
-
Study selection and evaluation were performed independently by multiple reviewers.
-
Study quality focused on:
-
Comparison of functional outcomes
-
Analysis of complication profiles across all treatment methods
-
Assessment Tools
-
Randomized studies evaluated using the Cochrane Risk of Bias Tool
-
Non-randomized studies evaluated using the Newcastle–Ottawa Scale
Outcome Measures
-
Functional outcomes:
-
American Orthopaedic Foot and Ankle Society score
-
Visual Analog Scale pain score
-
-
Complications:
-
Implant failure
-
Implant irritation
-
Infection
-
Reoperation
-
Statistical Analysis
-
Analysis performed using dedicated meta-analysis software.
-
Continuous outcomes reported as mean and standard deviation.
-
Categorical outcomes reported as event rates.
-
Mean differences used for functional scores.
-
Odds ratios used for complications.
-
Statistical significance defined as p ? 0.05.
Study Demographics
-
Total studies included: 21
-
Total patients: 1,059
-
Treatment distribution:
-
Dynamic fixation: 452 patients
-
Static fixation: 529 patients
-
Anatomic repair: 78 patients
-
Clinical Outcomes
Dynamic Fixation versus Static Fixation
-
Higher functional scores with dynamic fixation at:
-
3 months
-
1 year
-
-
Lower pain scores at 12 months
-
Interpretation:
-
Dynamic fixation provides superior short- and long-term functional outcomes compared to static fixation
-
Anatomic Repair versus Static Fixation
-
Higher functional scores with anatomic repair at:
-
6 months
-
1 year
-
-
Pain scores were similar between groups
-
Interpretation:
-
Anatomic repair improves functional recovery compared to static fixation
-
Dynamic Fixation versus Anatomic Repair
-
Higher functional scores with dynamic fixation at:
-
6 months
-
12 months
-
1 year
-
-
Slightly lower pain scores with anatomic repair at 12 months
-
Interpretation:
-
Dynamic fixation offers superior functional recovery, while anatomic repair may provide marginal pain relief at later follow-up
-
Complication Profile
Dynamic Fixation versus Static Fixation
-
Significantly fewer implant failures
-
Lower reoperation rates
-
No significant difference in infection or implant irritation
Anatomic Repair Comparison
-
No significant difference in implant-related complications compared to static fixation
-
Higher reoperation rates compared to dynamic fixation
Overall Findings
-
Dynamic fixation demonstrates:
-
Best functional outcomes
-
Lowest implant failure rates
-
Lowest reoperation rates
-
-
Anatomic repair shows:
-
Improved functional outcomes compared to static fixation
-
No clear advantage in complication reduction
-
-
Static fixation shows:
-
Higher rates of implant-related complications and reoperation
-
Comparison With Existing Evidence
-
Previous analyses have shown superior outcomes with dynamic fixation compared to static fixation.
-
Findings from this analysis are consistent with existing literature.
-
A major advantage of dynamic fixation is reduced risk of malreduction of the distal fibula within the tibial incisura.
Insights on Anatomic Repair
-
Evidence directly comparing anatomic repair with dynamic fixation is limited.
-
Available data suggest:
-
Earlier rehabilitation
-
Improved function in daily activities
-
-
Small sample size limits definitive conclusions.
Reasons for Superiority of Dynamic Fixation
-
Restores ligament continuity while stabilizing fractures
-
Permits physiologic micromotion
-
Allows earlier weight-bearing and rehabilitation
-
Results in:
-
Better functional recovery
-
Fewer complications
-
Lower reoperation rates
-
Study Limitations
-
Unequal sample sizes across treatment groups
-
Inconsistent outcome reporting
-
Inclusion of both randomized and observational studies
-
Variability in injury patterns and surgical techniques
-
Risk of bias related to:
-
Blinding
-
Allocation concealment
-
Incomplete data
-
-
Despite these limitations, pooled analysis reduces individual study bias.
Conclusion
-
Dynamic fixation demonstrates superior early clinical outcomes, fewer complications, and lower reoperation rates compared to static fixation and anatomic repair.
-
Long-term differences between treatment methods are minimal.
-
Anatomic repair provides better functional outcomes than static fixation but no clear advantage in complication rates.
Future Directions
-
Dynamic fixation appears to be the most effective overall treatment for acute ankle diastasis injuries.
-
Static fixation remains widely used but carries higher risks of hardware-related complications.
-
Anatomic repair is promising but requires further high-quality evidence.
-
Large, well-designed comparative studies with balanced sample sizes are needed to confirm long-term outcomes and cost-effectiveness.


Leave a Reply