Courtesy: Osama Kashlan MD, Associate Professor,
Weill Cornell Medicine, New York
Introduction
Endoscopic spine surgery has transformed the landscape of lumbar disc herniation treatment by enabling minimally invasive access to complex pathology. Using 6–7 mm incisions, surgeons can address even far-lateral or contralateral disc herniations. This article explores the nuances of interlaminar and transforaminal endoscopic approaches, based on a real case example and key surgical principles.
Endoscopic Reach and Access
The power of the endoscope lies in its ability to expand the decompression field with minimal invasiveness.
-
For example, even a disc herniation extending extraforaminally and across midline can be accessed and removed through a single, small incision.
-
While these surgeries take longer, the outcomes justify the time investment.
-
The access corridor created is wide enough to decompress comprehensively, preserving much of the surrounding anatomy.
Surgical Approaches: Transforaminal vs Interlaminar
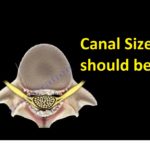
Visualizing the Access Pathways
Diagrams typically illustrate three primary approaches:
-
Transforaminal (SAP or TransSAP Approach): Docking at the superior articular process.
-
Transpar (Tubular-style Access): Similar to traditional tubular decompressions.
-
Interlaminar: Preferred in central or paracentral herniations, especially at L5–S1.
The endoscope “expands the box”, allowing far more reach and precision compared to traditional tubular surgery.
Case Study: Elderly Patient with Lumbar Stenosis and Scoliosis
Clinical Profile
-
Presentation: Left-sided upper lumbar radiculopathy.
-
Findings: Scoliosis with foraminal and lateral recess stenosis at L1–2 and L2–3.
-
Challenges:
-
Elderly patient with osteoporosis.
-
Poor candidate for a large surgery like multi-level XLIF.
-
Minimal back pain but significant nerve compression.
-
Surgical Strategy
-
L1–2: Endoscopic decompression.
-
L2–3: Tubular decompression due to prolonged time under anesthesia.
-
Patient was kept under general anesthesia, although such cases can be done awake.
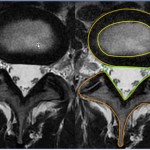
Postoperative Imaging
-
L1–2: Minimal bone resection with effective decompression (endoscopic).
-
L2–3: More bone removed (partial joint), yet similar clinical goal achieved (tubular).
-
Demonstrates the efficiency and anatomical preservation of endoscopic techniques.
Outcome
-
Excellent recovery.
-
The case underlined the importance of:
-
Balancing ideal technique with patient safety.
-
Recognizing one’s position on the learning curve.
-
Practicing “patient over ego” decision-making.
-
Key Surgical Takeaways
Which Lumbar Disc Herniations Can Be Treated Endoscopically?
Almost all.
-
Central and Paracentral Herniations:
-
Use interlaminar approach at L5–S1.
-
Also interlaminar from L1–L5 if ligamentum flavum hypertrophy is present.
-
-
No Ligamentous Hypertrophy:
-
Transforaminal approach is preferred.
-
Can decompress both dorsal and ventral aspects.
-
-
Foraminal and Extraforaminal Herniations:
-
If high iliac crest at L5–S1: Contralateral interlaminar.
-
Otherwise: Transforaminal or Transpars approaches are the workhorses.
-
Closing Thoughts by Dr. Kashlan
“This case reminded me to always consider where I am in the learning curve. If I were doing this today, I would have completed both levels endoscopically. But at that time, patient safety dictated a hybrid approach.”
Q&A: Concerns Around Endoscopic Spine Surgery
Q: Complication Rates in Endoscopic Surgery?
While endoscopic spine surgery offers:
-
Shorter recovery
-
Smaller incisions
-
Lower soft tissue trauma
…it also raises unique concerns, such as:
-
Seizures
-
Neurological dysfunction
-
Epidural hematomas
-
Incomplete decompression
Current Data Caveat:
-
Most studies come from high-volume expert centers (e.g., Korea).
-
Level 1 data is promising but may not be generalizable to all settings.
-
Surgeon experience and institutional readiness are key to success.
Conclusion
Endoscopic lumbar spine surgery is a powerful and evolving technique. With proper training and patient selection, it can match—and in many cases exceed—traditional surgery outcomes, while preserving anatomy and accelerating recovery. However, like any advanced technique, mastering it demands humility, patience, and continuous learning
Leave a Reply