Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Introduction
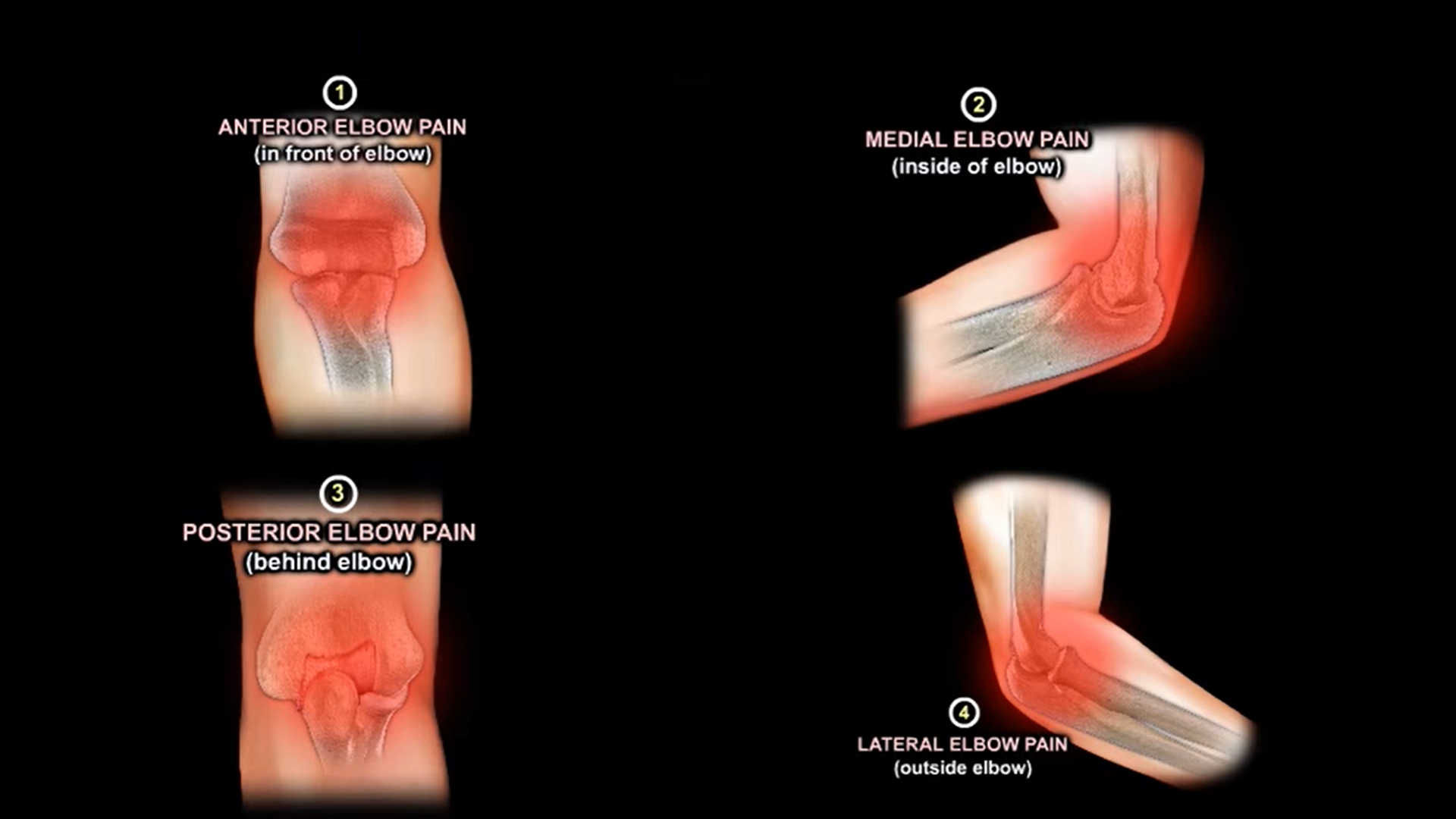
Elbow pain is best approached anatomically. Localizing the pain to a specific region of the elbow often helps narrow the diagnosis and guide treatment.
The elbow can be divided into four regions:
- Anterior (front)
- Medial (inner side)
- Posterior (back)
- Lateral (outer side)
This simple framework allows a systematic evaluation of patients presenting with elbow pain.
Anterior Elbow Pain
Distal Biceps Tendon Rupture
Mechanism
Typically occurs following a sudden eccentric load applied to a flexed elbow, such as lifting a heavy object.
Clinical Features
- Sudden onset pain in the front of the elbow
- Swelling and bruising
- Weakness during forearm supination
- Approximately 40% loss of supination strength
- Reverse Popeye deformity due to proximal tendon retraction
Treatment
Nonoperative
- Activity modification
- Physiotherapy
- Suitable for low demand individuals
Operative
- Tendon repair or reconstruction
- Preferred for active patients who require restoration of strength
Elbow Osteoarthritis
Causes
- Primary degenerative arthritis
- Post traumatic arthritis
Clinical Features
- Diffuse elbow pain
- Progressive stiffness
- Loss of range of motion
- Mechanical symptoms in advanced disease
Treatment
- Activity modification
- Nonsteroidal anti inflammatory medications
- Physiotherapy
- Intra articular injections
- Arthroscopic debridement
- Elbow arthroplasty in selected severe cases
Medial Elbow Pain
Medial Epicondylitis (Golfer’s Elbow)
Pathology
Overuse injury involving the flexor pronator origin at the medial epicondyle.
Clinical Features
- Pain over the medial epicondyle
- Symptoms aggravated by resisted wrist flexion
- Tenderness at the flexor origin
Treatment
- Rest and activity modification
- Physiotherapy
- Bracing
- Injections in selected cases
- Surgery for persistent symptoms
Cubital Tunnel Syndrome
Pathology
Compression of the ulnar nerve at the elbow.
Clinical Features
- Numbness and tingling in the little finger and ulnar half of the ring finger
- Weak grip strength
- Intrinsic muscle weakness in advanced cases
Treatment
- Avoid prolonged elbow flexion
- Night splinting
- Physiotherapy
- Ulnar nerve decompression or transposition when conservative treatment fails
Ulnar Collateral Ligament Injury
Pathology
Injury to the medial stabilizing ligament of the elbow.
Common in:
- Baseball pitchers
- Javelin throwers
- Other overhead athletes
Often referred to as the “Tommy John” injury.
Clinical Features
- Medial elbow pain
- Valgus instability
- Reduced throwing performance
Treatment
- Rest and rehabilitation
- Bracing
- Progressive return to sport
- Ulnar collateral ligament reconstruction in symptomatic athletes
Posterior Elbow Pain
Valgus Extension Overload Syndrome
Pathology
Repetitive valgus stress and terminal extension produce posterior impingement.
Commonly Seen In
- Throwing athletes
- Overhead sports participants
Clinical Features
- Pain during terminal extension
- Locking or clicking
- Reduced athletic performance
Treatment
- Activity modification
- Physiotherapy
- Anti inflammatory medications
- Arthroscopic debridement when symptoms persist
Olecranon Bursitis
Causes
- Repetitive minor trauma
- Direct injury
- Infection
Clinical Features
- Localized swelling over the tip of the elbow
- Tenderness
- Occasionally redness and warmth
Treatment
- Rest
- Ice application
- Anti inflammatory medications
- Aspiration when indicated
- Surgical excision in refractory cases
Lateral Elbow Pain
Lateral Epicondylitis (Tennis Elbow)
Pathology
Most commonly involves degeneration of the extensor carpi radialis brevis tendon.
Clinical Features
- Pain over the lateral epicondyle
- Pain with resisted wrist extension
- Reduced grip strength
Treatment
- Activity modification
- Ice and anti inflammatory medications
- Eccentric strengthening exercises
- Counterforce bracing
- Corticosteroid or PRP injections
- Surgery for resistant cases
Radial Tunnel Syndrome
Pathology
Compression of the radial nerve in the proximal forearm.
Clinical Features
- Pain distal to the lateral epicondyle
- May closely mimic tennis elbow
- Usually lacks significant tenderness directly over the epicondyle
Treatment
- Activity modification
- Physiotherapy
- Nerve gliding exercises
- Surgical decompression in persistent cases
Posterolateral Rotatory Instability (PLRI)
Pathology
Injury to the lateral collateral ligament complex leading to rotational instability.
Causes
- Trauma
- Recurrent elbow dislocations
- Excessive release during surgery for tennis elbow
Clinical Features
- Mechanical instability
- Clicking
- Apprehension during loading activities
Treatment
- Rehabilitation
- Bracing
- Ligament reconstruction when symptomatic instability persists
Clinical Pearls
Important Points
- Several elbow disorders can present with pain in the same anatomical region.
- A careful history and physical examination remain essential.
- Always compare findings with the opposite elbow.
- Assess for associated neurological symptoms.
- Use imaging appropriately when the diagnosis is uncertain.
Quick Memory Aid: A M P L
| Region | Common Causes |
|---|---|
| A | Anterior: Distal biceps rupture, Osteoarthritis |
| M | Medial: Golfer’s elbow, Cubital tunnel syndrome, UCL injury |
| P | Posterior: Valgus extension overload, Olecranon bursitis |
| L | Lateral: Tennis elbow, Radial tunnel syndrome, PLRI |
Take Home Message
When evaluating elbow pain, first determine the location of symptoms. Most common diagnoses can be rapidly narrowed using the Anterior, Medial, Posterior, Lateral (AMPL) approach, allowing focused examination, targeted investigations, and appropriate treatment.
Leave a Reply