Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Overview
-
Gout is a well-recognized cause of bursitis.
-
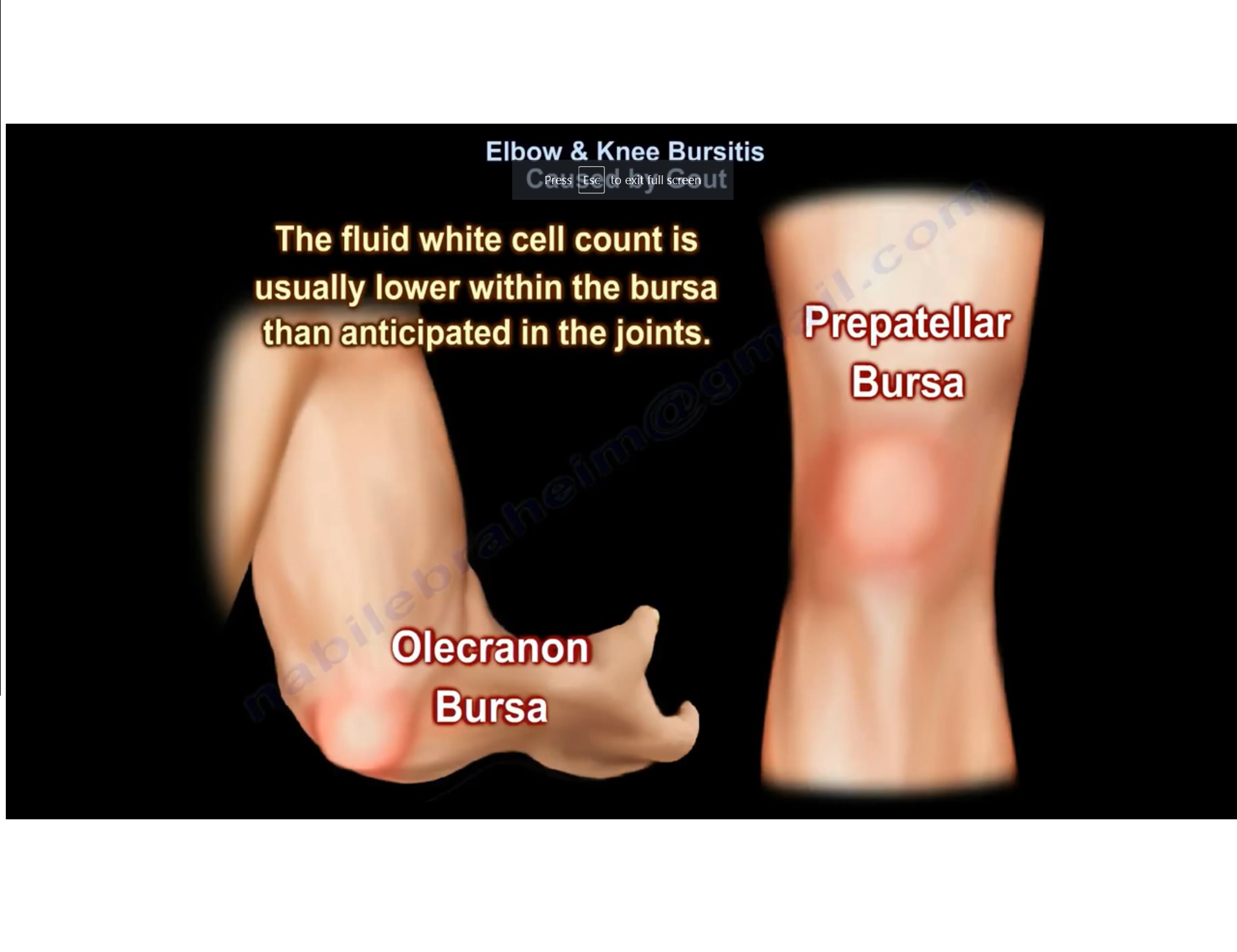
Gouty bursitis most commonly involves the olecranon bursa at the elbow and the prepatellar bursa at the knee.
Pathophysiology
-
In gouty bursitis, uric acid crystals are frequently present within the bursal fluid.
-
These crystals are needle-shaped and demonstrate negative birefringence under polarized light microscopy.
-
The presence of uric acid crystals within the bursa does not exclude concurrent infection.
Laboratory Findings
-
The white cell count in bursal fluid is usually lower than expected when compared with septic arthritis of a joint.
-
Despite lower cell counts, infection may still coexist and must be actively excluded.
Aspiration of the Bursa
-
Aspiration is essential for diagnostic evaluation.
-
Aspirated fluid should be sent for:
-
Culture and sensitivity
-
Cell count
-
Crystal analysis
-
Clinical Considerations
-
Gouty arthritis and bursitis may be bilateral.
-
These conditions can be difficult to treat, particularly in chronic or recurrent cases.
-
There is a recognized association between gouty bursitis and secondary infection, necessitating careful clinical and laboratory assessment.
Related Posts
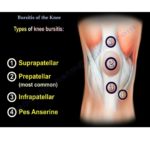 Bursitis of Knee
Bursitis of KneeCourtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
 Rheumatology Pearls
Rheumatology PearlsCourtesy: John M. Davis, III, MD, Division of Rheumatology Mayo Clinic
- Bursitis around the Hip
Courtesy: Prof Nabile Ebraheim, University of Toledo, OH, USA
Leave a Reply