Courtesy: Dr. Krishna Kiran, Dr Ashok Shyam, Ortho TV
Introduction
- Dual mobility systems are used in total hip replacement to reduce the risk of hip dislocation.
- They should not be considered a solution for poorly performed surgery.
- Proper surgical technique and accurate component positioning remain essential for stability.
Understanding Hip Stability in Arthroplasty
- The native hip joint rarely dislocates because the femoral head fits precisely within the acetabulum.
- During hip replacement, the removed femoral head is not completely replicated by the prosthetic head.
- Even when using a larger prosthetic head such as thirty six millimeters, there remains additional space within the joint.
- This increased space can predispose the artificial joint to instability, particularly when other factors such as spinopelvic abnormalities or improper component placement are present.
Considerations in Head Size and Implant Design
- The size of the acetabular component, bearing surface choice, and minimum polyethylene thickness influence the femoral head size that can be used.
- Current engineering limitations prevent polyethylene inserts from being manufactured below a safe thickness.
- A polyethylene thickness of approximately eight millimeters is generally maintained for safety.
- Extremely thin polyethylene or large hard bearing surfaces require caution because of potential long term complications.
Historical Background of Dual Mobility
- The dual mobility concept was introduced in nineteen seventy nine.
- It combines two established principles of hip replacement:
- Low friction arthroplasty.
- Large diameter head articulation.
- The design includes:
- A metallic acetabular cup with a polished internal surface.
- A small femoral head attached to the femoral stem.
- A large polyethylene liner that articulates with the metal cup.
Modern Design Features
- Current implants often include ceramic femoral heads and highly cross linked polyethylene liners.
- Some designs allow the use of fixation screws to improve cup stability.
- Modular metal liners are also available, allowing flexible screw placement during surgery.
- However, modular systems may carry a risk of metal debris formation due to micro movement between metal components.
Advantages of Dual Mobility
- Dual mobility systems increase the effective head size of the hip prosthesis.
- Larger effective head size improves joint stability and reduces the likelihood of dislocation.
- They partially compensate for the loss of the native femoral head size in conventional hip replacement.
Situations Where Dual Mobility is Commonly Used
Dual mobility implants are particularly useful in patients at high risk of hip instability, including:
- Elderly individuals with fracture of the femoral neck who require total hip replacement.
- Patients undergoing surgery through posterior surgical approaches.
- Cases with intertrochanteric fractures combined with pre existing hip arthritis.
- Failed fixation procedures such as failed proximal femoral nail with acetabular damage.
- Revision hip replacement performed for recurrent dislocation.
- Patients with neuromuscular disorders affecting hip stability.
- Situations with abductor muscle deficiency.
- Revision surgeries after complex femoral resections.
Surgical Considerations
- Correct assembly of the femoral head within the polyethylene liner is essential.
- The components usually lock together with a snapping mechanism.
- Improper assembly can result in disengagement of the articulation and implant failure.
Limitations and Unanswered Questions
- Although dual mobility implants reduce dislocation risk, they do not completely eliminate it.
- Long term outcomes and survivorship data are still evolving.
- Achieving adequate fixation of the acetabular component can be difficult in osteoporotic bone.
- The long term performance of metal backed cemented cups remains uncertain.
Implant Related Concerns
- Dual mobility systems have multiple articulating surfaces, which may increase the theoretical risk of wear.
- The polyethylene liner articulates both with the femoral head and the metal cup.
- Higher volumetric wear may occur compared with traditional designs.
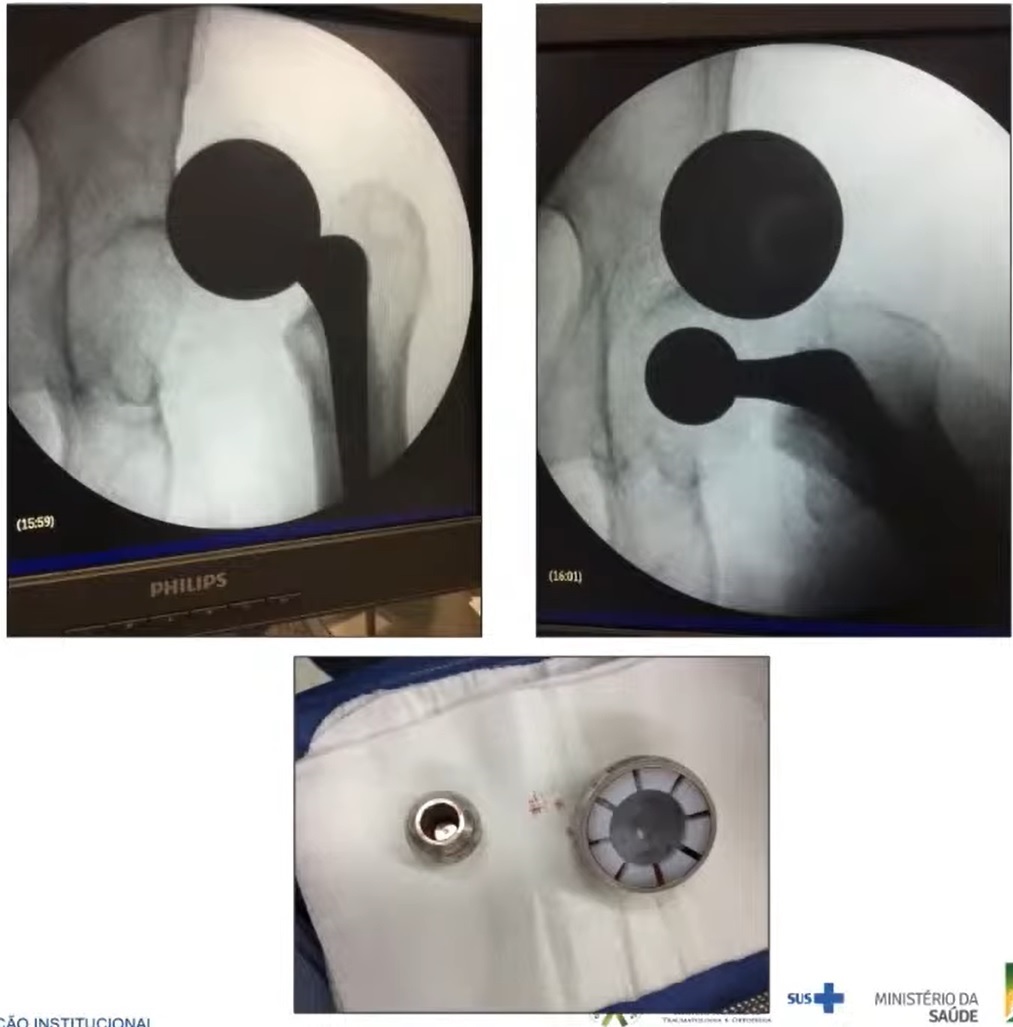
Unique Complication: Intraprosthetic Dislocation
- A distinctive complication associated with dual mobility implants is intraprosthetic dislocation.
- In this condition, the femoral head disengages from the polyethylene liner while the liner remains inside the acetabular cup.
- This complication usually develops several years after surgery due to progressive polyethylene wear or failure of the retention mechanism.
Radiological Features
- Radiographs may show eccentric positioning of the femoral head within the acetabular component.
- A characteristic “bubble sign” may also be visible.
- Attempting closed reduction in such cases may not be successful.
Types of Intraprosthetic Dislocation
Common mechanisms include:
- Failure of the polyethylene retention mechanism caused by long term wear.
- Arthrofibrosis leading to restricted movement at the articulation interfaces.
- Loosening of the acetabular component.
Additional Potential Complications
- Polyethylene wear and osteolysis.
- Aseptic loosening of the implant.
- Metallosis due to metal debris in modular systems.
- Increased wear risk in young and highly active patients.
Considerations in Young Patients
- Younger patients may experience greater implant wear because of higher activity levels.
- Patients below fifty years of age or those treated for childhood hip diseases may have increased long term risks.
- Therefore routine use of dual mobility implants in young patients is not strongly supported by current evidence.
Clinical Practice Recommendations
- Dual mobility implants are best reserved for patients with a high risk of postoperative instability.
- They are particularly useful in elderly individuals or complex revision surgeries.
- Surgeons should avoid routine use in low risk patients without clear indications.
Leave a Reply