Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Distal Femoral Physeal Fractures (Pediatric)
Overview
- Injury to the distal femoral physis in children
- One of the most important pediatric knee injuries
Clinical Importance
- High risk of growth arrest (~50–60%)
- Risk increases with:
- Displacement
- High-energy trauma
Key Clinical Point
- In children presenting with:
- Suspected MCL/LCL injury
Rule Out
- Distal femoral physeal fracture
Anatomy and Growth Facts
Growth Contribution
- ~70% of femoral growth
- ~37% of total lower limb growth
Growth Rate
- ~9 mm/year
Ossification
- First epiphysis to ossify
- Last to fuse
Fusion Age
- Girls: ~14 years
- Boys: ~16 years
Salter–Harris Classification
Most Common Type
- Salter-Harris Type II
Key Feature
Thurston–Holland Fragment
- Triangular metaphyseal fragment
- Helps identify SH Type II fracture
Pathophysiology
- Weakest area of physis:
- Zone of hypertrophy
Special Feature (Distal Femur)
- Fracture often crosses:
- Multiple physeal zones
Growth Occurs At
- Metaphyseal side of physis
Management Principles
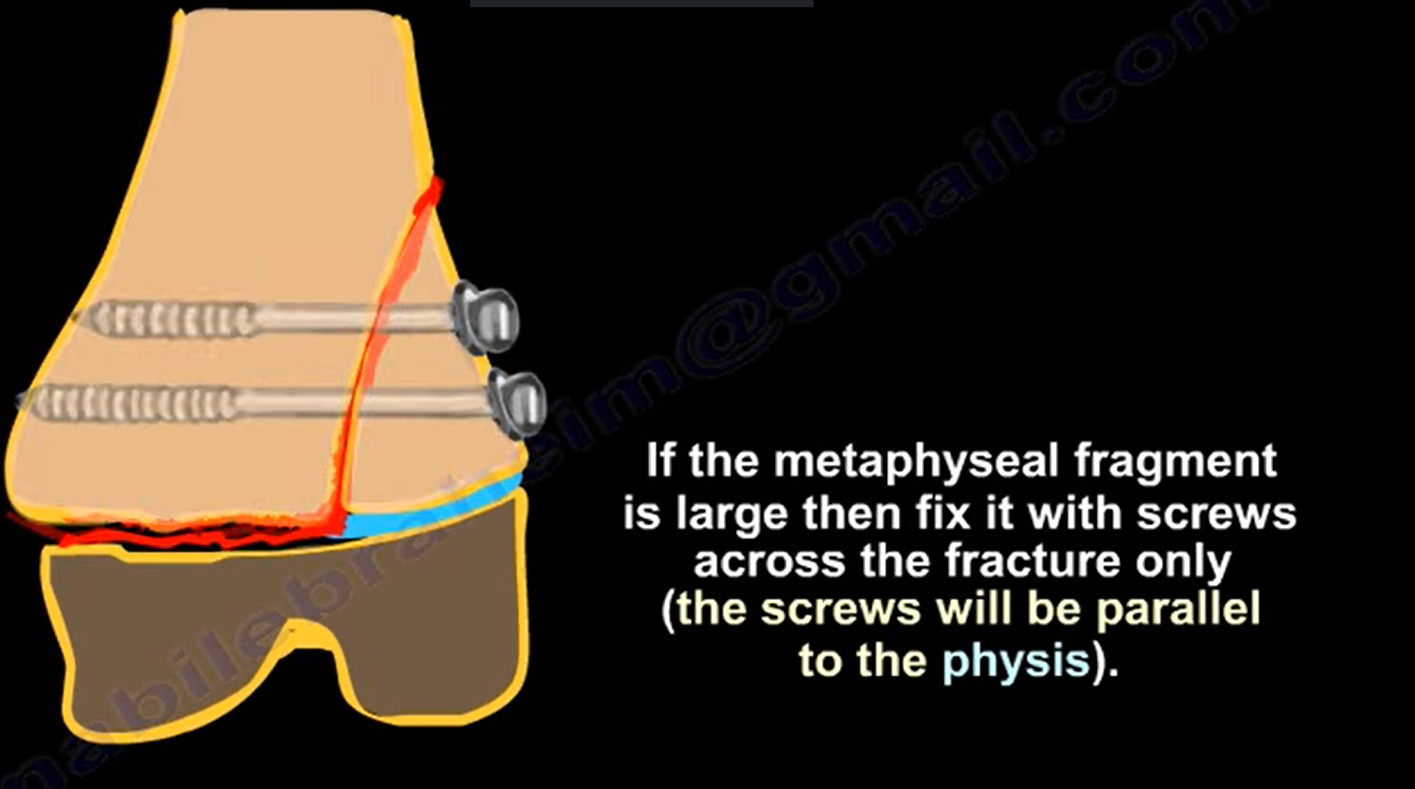
1. Large Metaphyseal Fragment (SH II)
- Fixation with:
- Screws
Technical Points
- Screws:
- Parallel to physis
- Avoid physeal damage
2. Small Fragment / Salter I
- Closed reduction
- Percutaneous fixation
Implant
- Smooth K-wires
3. Occult Injury
Scenario
- Normal X-ray but high suspicion
Next Step
- MRI or CT scan
When to Suspect
- Painful knee
- Instability
- Pediatric patient
Growth Arrest Patterns
1. Central Arrest
- Leads to:
- Limb length discrepancy (LLD)
2. Peripheral Arrest
- Leads to:
- Angular deformity
Examples
- Medial arrest – Genu valgum
- Lateral arrest – Genu varum
Management of Growth Arrest
< 50% Physis Involved
- Physeal bar resection
- Fat interposition
> 50% Physis Involved
- Epiphysiodesis
- Growth modulation
Clinical Prediction Examples
- 12-year-old:
- ~2 cm shortening expected
- 13-year-old:
- ~3 cm predicted – consider intervention
Special Points
- Minimal shortening if injury occurs:
- Within 2 years of skeletal maturity
Risk
- Younger children:
- Higher likelihood of repeat surgery (8×)
Deformity Prediction Trick
Based on Thurston–Holland Fragment
- Spike lateral – medial physis injured – Varus deformity
- Spike medial – lateral physis injured – Valgus deformity
Key Exam Pearls
- Most common type:
- Salter-Harris Type II
- Most serious complication:
- Growth arrest
- Best investigation (occult injury):
- MRI
Treatment Summary
- Large fragment – Screws
- Small fragment – K-wires
Critical Clinical Rule
- Always suspect physeal injury in:
- “Ligament injuries” in children

Leave a Reply