Courtesy: Pierre Lamaunorie, Tolouse, France
Distal Biceps Tendon Ruptures
Overview
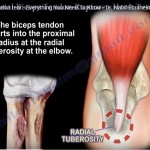
Distal biceps tendon ruptures are relatively uncommon injuries that typically occur during an eccentric contraction of the biceps muscle, often with the elbow in a semi-flexed position. Although frequently perceived as isolated traumatic events, these injuries usually result from a combination of chronic tendon degeneration and an acute overload.
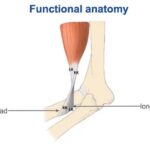
Anatomy of the Distal Biceps Tendon
Tendon Anatomy
The distal biceps consists of two distinct tendon components:
- Long Head
- Short Head
These tendon components have separate insertions on the radial tuberosity:
- Short head: Inserts slightly more distal and posterior
- Long head: Inserts more proximal
Understanding this anatomy is essential for accurate diagnosis and anatomic surgical repair.
Blood Supply
The distal biceps tendon receives its vascular supply from:
- Brachial artery
- Recurrent radial artery
Three Vascular Zones
- Proximal vascular zone
- Middle critical zone
- Poor intrinsic blood supply
- Most susceptible to ischemia and degeneration
- Distal vascular zone
The relatively hypovascular middle zone is believed to contribute significantly to tendon degeneration and rupture.
Epidemiology
- Represents 3–5% of all peripheral tendon ruptures
- Incidence:
- Approximately 4 cases per 100,000 population annually
- Bilateral ruptures occur in 5–10% of patients.
- Most injuries occur between 35 and 65 years, with an average age of approximately 46 years.
Risk Factors
Distal biceps tendon rupture is usually multifactorial.
Mechanical Factors
- Repetitive pronation
- Chronic tendon degeneration
- Radial tuberosity impingement
- Bony spurs
- Previous distal biceps tendinopathy
Repeated pronation decreases the radioulnar space, promoting chronic tendon wear and eventual rupture.
Patient-Related Risk Factors
- Age >40 years
- Obesity (BMI ?30)
- Smoking
- Anabolic steroid use
- High-demand athletic activity
Smoking increases the risk of rupture by 2–3 times due to impaired collagen quality and reduced tendon vascularity. Anabolic steroids create a mismatch between muscle strength and tendon capacity, increasing susceptibility to rupture.
Clinical Presentation
Patients commonly present with:
- Sudden pain in the antecubital fossa
- Audible “pop” at the time of injury
- Weakness of elbow flexion
- Weakness of forearm supination
- Bruising around the elbow
- Reverse Popeye deformity (occasionally)
Many patients report preceding episodes of distal biceps tendinopathy before complete rupture.
Clinical Examination
Hook Test
The Hook Test is considered the most reliable clinical examination for complete distal biceps rupture.
Technique
- Shoulder abducted
- Elbow flexed to 90°
- Forearm fully supinated
- Examiner attempts to hook the lateral edge of the tendon with the index finger
Interpretation
- Normal: Tendon can be hooked
- Positive Test: Tendon cannot be palpated or hooked, indicating complete rupture
Reported sensitivity approaches 100% for complete tears.
Evaluation of Partial Tears
Partial ruptures may produce:
- Persistent anterior elbow pain
- Pain during resisted elbow flexion
- Increased pain during resisted flexion with forearm pronation
Because part of the tendon remains intact, the Hook Test may be falsely negative in partial tears.
Imaging
MRI
MRI is the imaging modality of choice for distal biceps injuries.
Advantages
- Accurate diagnosis of complete ruptures
- Identification of partial tears
- Assessment of tendon degeneration
- Surgical planning
MRI demonstrates substantially greater diagnostic accuracy than ultrasound.
Ultrasound
Although widely available, ultrasound has significantly lower diagnostic accuracy and is generally not recommended as the primary imaging modality for distal biceps tendon rupture.
Management of Partial Tears
Treatment depends on:
- Percentage of tendon involvement
- Functional demands
- Patient expectations
Conservative Management
Appropriate for:
- Low-demand patients
- Small partial tears
- Mild symptoms
Treatment includes:
- Activity modification
- Physiotherapy
- Gradual return to activity
Surgical Management
Generally recommended for:
- Tears involving more than 50% of the tendon
- Persistent symptoms despite conservative treatment
- High-demand athletes
Many surgeons advocate complete release of the remaining tendon followed by anatomic reinsertion.
Surgical Repair
Cortical Button Fixation
Cortical button fixation has become the preferred technique for acute distal biceps repair.
Advantages
- Strong tendon-to-bone fixation
- High biomechanical strength
- Early rehabilitation
- Reliable anatomic restoration
Compared with suture anchors, cortical button fixation demonstrates higher load-to-failure values, making it particularly suitable for active individuals and athletes.
Surgical Technique
Key surgical steps include:
- Small anterior incision
- Identification and protection of the lateral antebrachial cutaneous nerve
- Retrieval of the ruptured tendon
- Tendon preparation using high-strength suture
- Preparation of the radial tuberosity
- Cortical button insertion
- Anatomic tendon reinsertion
- Secure fixation under appropriate tension
Attention to surgical technique helps optimize fixation strength while minimizing complications.
Postoperative Rehabilitation
Early mobilization is emphasized.
Rehabilitation Principles
- No prolonged immobilization
- Immediate active range of motion
- Avoid passive stretching during the early phase
- Progressive strengthening based on healing
Typical Recovery Timeline
- 0–3 weeks: Minimal loading
- 6 weeks: Gradual strengthening (up to approximately 7 kg)
- 6 weeks onward: Progressive unrestricted strengthening
- 6 months: Expected return to full function and athletic performance
Outcomes
Following surgical repair:
- Approximately 95% of patients return to sport.
- Recovery of elbow flexion and supination strength reaches 92–96% in most patients.
Elite athletes may experience reduced rates of return to pre-injury performance levels, highlighting the importance of timely diagnosis and optimal surgical management.
Management of Chronic Ruptures
Chronic ruptures present additional challenges due to tendon retraction and scarring.
Acute Repairs
- Best performed within 2 months of injury whenever feasible.
Chronic Injuries
When primary repair is not possible:
- Achilles tendon allograft reconstruction is a reliable option.
- Tendon grafting allows restoration of length and function in markedly retracted tears.
Complications
Potential complications include:
- Lateral antebrachial cutaneous nerve paresthesia
- Superficial radial nerve sensory disturbance
- Posterior interosseous nerve injury (rare with meticulous technique)
- Hematoma
- Infection
- Heterotopic ossification
Most sensory nerve symptoms are transient and resolve with time. Delayed surgery may increase minor wound-related complications, while repairs beyond six weeks become technically more demanding because of tendon retraction.
Key Takeaways
- Distal biceps tendon rupture is usually the result of chronic degeneration combined with an acute eccentric load.
- The Hook Test remains the most reliable clinical examination for complete tears.
- MRI is the preferred imaging modality for diagnosis and surgical planning.
- Surgical repair is generally recommended for complete ruptures, high-demand patients, and symptomatic partial tears involving more than 50% of the tendon.
- Cortical button fixation provides strong, reliable fixation and supports early rehabilitation.
- Early diagnosis, meticulous surgical technique, and structured rehabilitation are essential to optimize functional recovery and facilitate return to sport.


Leave a Reply