Courtesy: Prof Nabil Ebraheim, Unviersity of Toledo, Ohio, USA
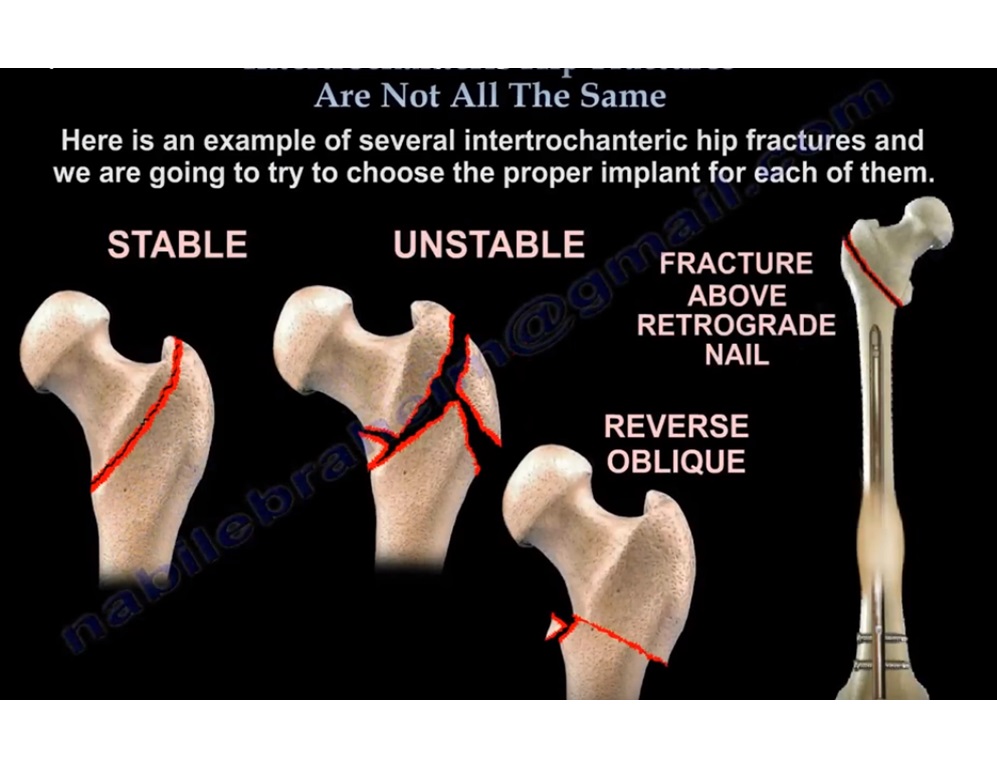
Appropriate implant selection in intertrochanteric hip fractures depends on fracture stability, fracture pattern, and integrity of the lateral wall. Correct assessment directly influences fixation stability and clinical outcomes.
1. Stable Intertrochanteric Fractures
(Regular fracture pattern)
-
Stable fracture patterns show comparable clinical outcomes with:
-
Sliding hip screw
-
Intramedullary nail
-
-
Sliding hip screw is a cost-effective option with equivalent results in stable fractures.
-
A fixation construct using 2 screws provides outcomes equivalent to constructs using 3 or 4 screws.
High-Energy Stable Fractures
-
In fractures caused by high-energy trauma:
-
Initial traction should be applied
-
If acceptable alignment is achieved with traction, closed fixation may proceed
-
If alignment is not achieved, open reduction is required
-
-
Compression hip screw fixation is appropriate when:
-
Displacement is significant
-
Comminution is minimal
-
2. Unstable Intertrochanteric Fractures
(Irregular or unstable fracture pattern)
-
Unstable fracture patterns should be treated with a cephalomedullary nail.
-
These fractures are prone to collapse and medialization, making extramedullary fixation less reliable.
3. Reverse Oblique Intertrochanteric Fractures
-
Reverse oblique fracture patterns require cephalomedullary nailing.
-
Sliding hip screw fixation has a high failure rate in these fractures due to:
-
Lack of lateral buttress
-
Excessive shear forces across the fracture site
-
4. Fracture Proximal to a Retrograde Femoral Nail
-
Recommended management is:
-
Fracture reduction and internal fixation using a compression hip screw
-
-
Antegrade intramedullary nailing is not feasible unless:
-
The retrograde nail is removed
-
-
Removal of the retrograde nail represents a larger and more invasive procedure and is generally avoided when possible.
Role of the Lateral Wall in Implant Selection
-
The integrity of the lateral wall is a critical predictor of fracture stability.
-
A thin or incompetent lateral wall:
-
Increases the risk of intraoperative lateral wall blowout
-
Leads to higher rates of postoperative fixation failure
-
Increases the likelihood of reoperation
-
Key Radiographic Considerations
-
If the lateral wall thickness is less than 20 millimeters:
-
Compression hip screw fixation should be avoided
-
The fracture should be treated as unstable
-
Cephalomedullary nailing is preferred
-
-
Lateral wall integrity is an important radiographic sign guiding implant choice and predicting outcomes.

Leave a Reply