Courtesy: Dr Amr Abdelgawad, University of Texas,USA
Definition
Developmental dysplasia of the hip (DDH) encompasses a spectrum of abnormalities ranging from:
-
Acetabular dysplasia
-
Hip subluxation
-
Complete dislocation of the femoral head
These abnormalities may be present at birth or develop during infancy.
Epidemiology
-
Incidence: 1–2 per 1,000 live births
-
True dislocation: approximately 1 per 1,000 infants
-
Left hip is more commonly affected
-
May be associated with other conditions related to restricted intrauterine space, such as:
-
Metatarsus adductus
-
Torticollis
-
Risk Factors
-
Female sex
-
First-born child
-
Breech presentation
-
Positive family history of DDH
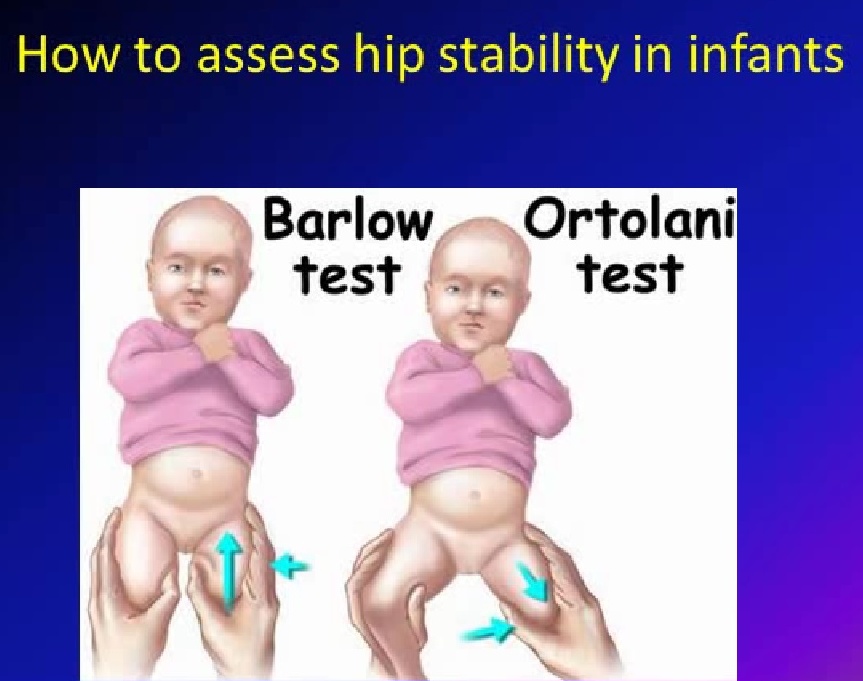
Clinical Examination in Newborns
Barlow Test
-
Assesses whether the hip is subluxable
-
Hip is flexed and adducted with posterior pressure
-
A positive test indicates an unstable hip
Ortolani Test
-
Assesses whether the hip is dislocated but reducible
-
Gentle abduction with anterior lifting force
-
A palpable or audible “clunk” indicates reduction of the femoral head into the acetabulum
Ultrasound Evaluation
-
Performed with the hip and knee flexed
-
Transducer placed over the greater trochanter
-
Based on Graf method
Key Angles
-
Alpha angle
-
Assesses bony acetabular coverage
-
Larger angle = better coverage
-
-
Beta angle
-
Reflects cartilaginous roof
-
Larger angle = increased risk of subluxation
-
American Academy of Pediatrics (AAP) Recommendations for DDH Screening
Universal Screening
-
All newborns should undergo physical examination
-
Routine ultrasound for all newborns is not recommended
Positive Ortolani or Barlow Test (Definite Clunk)
-
Immediate orthopaedic referral
-
No need for ultrasound or radiographs
-
Triple diapering is not recommended (delays effective treatment)
Equivocal Findings (Soft click or asymmetry)
-
Repeat physical examination after 2 weeks
At 2-week follow-up:
-
Findings unchanged – orthopaedic referral or ultrasound
-
Findings resolved – no further action
-
Definite clunk – orthopaedic referral
Role of Risk Factors When Newborn Exam Is Normal
-
Female infants
-
Re-examine hips at 2 weeks
-
-
Positive family history or breech presentation
-
Boys: re-evaluation at 2 weeks
-
Girls:
-
Ultrasound at 6 weeks
-
Radiograph at 4 months
-
-
-
All breech infants (boys and girls):
-
Consider pelvic radiographs at 4 months to assess acetabular development
-
Periodic Hip Examination
-
Hip examination must be performed at every well-baby visit
-
If DDH is suspected at any age (abnormal exam or parental concern such as difficulty changing diapers), one of the following is required:
-
Focused hip examination in a relaxed child
-
Orthopaedic referral
-
Imaging:
-
Ultrasound if <4 months
-
Radiographs if >4 months
-
-
Assessment in Toddlers and Older Children
-
Galeazzi sign: femoral shortening with knees flexed
-
Asymmetrical gluteal or thigh folds
-
Limited hip abduction
-
Gait abnormalities:
-
Limp (unilateral DDH)
-
Waddling gait (bilateral DDH)
-
Pain is never a symptom of untreated DDH until secondary osteoarthritis develops, typically in adulthood.
Radiographic Assessment
Hilgenreiner’s Line
-
Horizontal line through both triradiate cartilages
-
Femoral head ossification center should lie below this line
Perkin’s Line
-
Perpendicular line at the lateral edge of the acetabulum
-
Femoral head ossification center should lie medial to this line
Shenton’s Line
-
Smooth arc along inferior femoral neck and superior obturator foramen
-
Should be continuous
Normal Hip
-
Ossification center lies in the inferomedial quadrant
Treatment of DDH
Birth to 4–6 Months
-
Pavlik harness
-
Keeps hip:
-
Flexed 90–100° (anterior straps)
-
Gently abducted (posterior straps)
-
-
Distance between knees: 3–4 finger breadths (avoid excessive abduction)
-
Worn 23 hours/day
-
Duration: age at application + 2 months
After 6 Months
-
Arthrogram
-
Closed reduction under anesthesia
-
Hip spica cast
Missed DDH After 18 Months
-
Requires open reduction
-
May need:
-
Femoral osteotomy
-
Pelvic osteotomy
-
-
Outcomes less predictable
Complications
-
Avascular necrosis (AVN) of the femoral head
-
Can occur with any form of treatment
-
Risk increases with:
-
Excessive abduction
-
Forceful or repeated reductions
-
-
May result in pain and early degenerative arthritis
Key Take-Home Messages
-
DDH is a spectrum, not a single condition
-
Clinical examination is the cornerstone of screening
-
Imaging complements but does not replace physical examination
-
Early diagnosis allows simple and effective treatment
-
Delayed or missed DDH leads to complex surgery and poorer outcomes
Leave a Reply