Current Concepts in Treating Meniscal Injuries
Introduction
Management of meniscal injuries has evolved significantly over the past few decades. Earlier treatment philosophies favored meniscectomy, but increasing understanding of meniscal biomechanics and long-term joint preservation has shifted modern practice toward meniscal preservation whenever possible.
Current treatment strategies emphasize:
- Preservation of meniscal tissue
- Restoration of knee biomechanics
- Prevention of early osteoarthritis
- Evidence-based patient selection
The “Pendulum of Knowledge” in Meniscus Treatment
Medical knowledge often evolves like a pendulum:
- Foundational understanding
- Introduction of new concepts
- Development of dogma
- Re-evaluation through evidence
- Balanced modern approach
This concept strongly applies to the evolution of meniscus treatment.
Historically:
- The meniscus was considered a vestigial structure
- Meniscectomy was routinely performed
Modern evidence has demonstrated that:
- Meniscal loss significantly increases the risk of osteoarthritis
As a result, treatment philosophy has shifted toward:
- “Save the meniscus whenever possible”
Meniscus Anatomy and Structure
Histology
The meniscus is composed predominantly of:
- Type I fibrocartilage
It contains:
- Relatively low water content
Nutrition
Meniscal nutrition occurs through:
- Diffusion from synovial fluid
- Peripheral vascular supply
Functional Anatomy
The meniscus is wedge-shaped, which helps:
- Improve joint congruency
- Enhance load distribution
Major functions include:
- Shock absorption
- Load transmission
- Joint stabilization
- Secondary support for ACL and PCL stability
Fiber Orientation
Circumferential Fibers
Also called:
- Hoop fibers
These resist:
- Compressive forces
Radial Fibers
These maintain:
- Structural integrity of the meniscus
Loss of hoop stress results in:
- Functional loss of the meniscus
Biomechanical Importance of the Meniscus
The meniscus plays a critical role in knee biomechanics.
Functions include:
- Increasing contact area between femur and tibia
- Reducing focal stress
- Improving force distribution
The meniscus converts:
- The relatively flat tibial plateau
- Into a more congruent articulation with the femoral condyle
Loss of meniscal tissue causes:
- Increased contact pressure
- Accelerated cartilage degeneration
- Early osteoarthritis
Clinical Examination Pearls
Meniscal Mobility
The lateral meniscus is:
- More mobile than the medial meniscus
which explains why:
- The medial meniscus is more commonly injured
Mechanical Symptoms
A “click” alone does not confirm meniscal pathology.
A clinically significant meniscal test should reproduce:
- Pain
- Mechanical symptoms
together.
Evolution of Meniscus Treatment
Historical Approach
Older surgical philosophy considered the meniscus:
- Functionally unimportant
leading to:
- Routine meniscectomy
Shift in Understanding
Long-term studies demonstrated:
- Increased osteoarthritis following meniscectomy
This changed treatment philosophy toward:
- Meniscal preservation
Current Standard
Modern principles recommend:
- Repair whenever feasible
especially in:
- Young patients
- Peripheral tears
- Associated ACL injuries
Meniscal Repair Outcomes
Better healing outcomes are associated with:
- ACL reconstruction
- Peripheral vascular tears
- Simple vertical longitudinal tears
Healing rates may reach:
- Approximately 93–94% when combined with ACL reconstruction
Poor Prognostic Factors
Less favorable healing occurs in:
- Complex tears
- Degenerative tears
- Central avascular zone injuries
Relationship Between ACL and Meniscus
Untreated ACL deficiency significantly increases the risk of meniscal injury.
Important associations include:
- Fivefold increase in meniscal tears
- Sixfold increase in osteoarthritis risk
- Sixteenfold increase in total knee arthroplasty risk
ACL reconstruction helps:
- Improve meniscal healing
- Prevent further meniscal damage
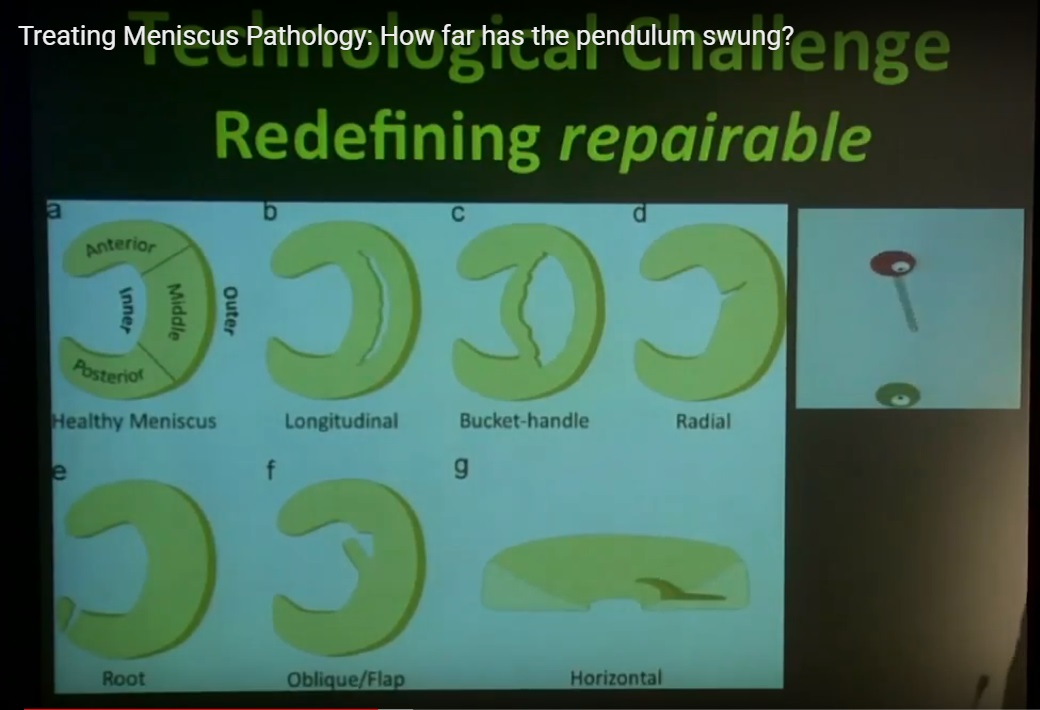
Expanding Indications for Meniscal Repair
Modern concepts have expanded the definition of:
- “Repairable meniscus”
Radial Tears
Previously:
- Routinely resected
Current evidence suggests repair may:
- Reduce contact stress
- Restore near-normal biomechanics
Horizontal Tears
Horizontal cleavage tears can lead to:
- Increased contact pressure
- Reduced contact area
Repair techniques such as:
- Sandwich repair techniques
may help restore function.
Meniscal Root Tears
Meniscal root tears behave biomechanically like:
- Total meniscectomy
Root repair may:
- Improve clinical outcomes
However:
- Incomplete healing
- Persistent meniscal extrusion
remain common concerns.
Iatrogenic Meniscal Injury
Meniscal injury may occur during ACL reconstruction.
Potential causes include:
- Tunnel malposition
- Improper drill angle
This highlights the importance of:
- Precise surgical technique
Meniscus Restoration Techniques
Mesenchymal Stem Cells (MSC)
Potential benefits include:
- Symptom improvement
- Increased meniscal volume on MRI
Limitations of MSC Therapy
Current limitations include:
- Poor-quality evidence
- Unknown long-term durability
- No proven prevention of osteoarthritis
Meniscal Scaffolds
Scaffolds provide:
- A framework for tissue regeneration
Reported benefits include:
- Increased meniscal volume
- Functional improvement
Limitations of Scaffolds
- Mixed clinical evidence
- Uncertain long-term outcomes
Meniscal Allograft Transplantation (MAT)
Indications
MAT is considered in:
- Young symptomatic patients
- Meniscal deficiency
- Minimal osteoarthritis
Outcomes
Potential benefits include:
- Pain reduction
- Improved stability
- Approximately 77% return to sports
Limitations
Common limitations include:
- Meniscal extrusion
- Lack of proven osteoarthritis prevention
- Limited role as a prophylactic procedure
Degenerative Meniscal Tears
Epidemiology
Degenerative meniscal tears increase with age.
Approximate prevalence:
- 20% in patients in their 50s
- 35% in patients in their 60s
- 50% by age 70
Evidence from Randomized Trials
Studies comparing arthroscopy with:
- Sham surgery
- Physiotherapy
have shown:
- No significant difference in many degenerative tears
Important Clinical Insight
Arthroscopic surgery may have a:
- Significant placebo effect
This reinforces the importance of:
- Careful patient selection
Current Management Algorithm
Initial Non-Operative Treatment
For degenerative tears without true mechanical locking:
- Physiotherapy
- NSAIDs
- Activity modification
- Injections when appropriate
should be the first-line treatment.
Reassessment
Patients are typically reassessed after:
- Approximately 3 months
Surgery may be considered if symptoms persist.
Presence of Osteoarthritis
If significant arthritis is present:
- Management should focus primarily on osteoarthritis treatment rather than meniscal surgery.
Clarifying Mechanical Symptoms
True Locking
True locking means:
- The joint becomes physically stuck
Not True Locking
The following are not considered true locking:
- Clicking
- Pain inhibition
- Transient catching sensations
This distinction is critical for surgical decision-making.
Key Clinical Principles
What Is Well Established
- The meniscus is essential for knee health.
- Meniscal loss accelerates osteoarthritis.
- Preservation is preferable whenever possible.
Current Treatment Philosophy
- Repair is preferred over resection.
- Combined ACL reconstruction improves healing.
- Degenerative tears should initially be managed conservatively.
Current Grey Zones
Areas that continue to evolve include:
- Radial tear repair
- Horizontal tear management
- Root tear outcomes
- Biologics and scaffold use
- Optimal timing for meniscal transplantation
Final Take-Home Message
Modern meniscus treatment focuses on preservation rather than removal.
Successful management requires:
- Understanding meniscal biomechanics
- Appropriate patient selection
- Evidence-based surgical indications
- Long-term joint preservation strategies
Treatment decisions should balance:
- Symptoms
- Functional demands
- Risk of osteoarthritis
- Short-term recovery
- Long-term outcomes
A balanced, evidence-based approach remains the key principle in contemporary meniscal surgery.
Courtesy: Dr Mark Hutchinson, Visiting Orthopaedic Surgeon – Aspetar

Leave a Reply