Courtesy: Dr A Reddy, Ashok Shyam TV, Ortho
Introduction
-
Focus: Cruciate-retaining (CR) total knee arthroplasty.
-
Personal practice preference:
-
~99% of primary TKAs performed as CR knees.
-
Used even in severe deformities.
-
-
Transition from posterior-stabilized (PS) to CR:
-
Smaller knee sizes.
-
Thinner femoral condyles.
-
Concerns regarding box cuts in smaller bone stock.
-
Why Choose Cruciate Retaining?
Surgical Advantages
-
No box cut required:
-
Preserves bone stock.
-
Shorter operative time.
-
Reduced risk of condylar fracture in small knees.
-
-
Better bone available if revision becomes necessary.
Design-Related Concerns in Posterior-Stabilized Knees
-
Patellar clunk syndrome (primarily seen in PS designs).
-
Post-cam dislocation.
-
Cam wear.
-
Limited tolerance to hyperextension.
-
Trial post vulnerability to wear from rotational malalignment.
-
Rotational mismatch may occur:
-
Intraoperatively.
-
Dynamically during gait.
-
Biomechanical Advantages of CR Knee
-
Preserves posterior cruciate ligament (PCL).
-
Maintains more physiologic joint line.
-
Better quadriceps efficiency.
-
Improved stair-climbing mechanics (reported in literature).
-
PCL contributes to:
-
Posterior stability.
-
Varus-valgus stability.
-
-
Reduced constraint compared to PS designs.
-
Potentially lower joint reaction forces.
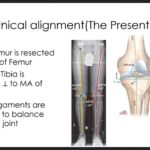
Joint Line Considerations
-
If PCL is sacrificed:
-
Flexion gap increases (~5 mm).
-
May require additional distal femoral resection.
-
Joint line elevation can occur.
-
Risk of mid-flexion instability increases.
-
CR design:
-
Maintains joint line more consistently.
-
Less risk of mid-flexion instability.
Addressing the “PCL is Non-Functional” Argument
-
PCL does not need to be completely normal to be retained.
-
Majority of primary TKAs can successfully preserve PCL with minor balancing.
When to Consider PCL Balancing
Clinical features predicting need for balancing:
-
Limited preoperative range of motion.
-
Flexion contracture.
-
Significant varus or valgus deformity.
Essential Steps Before Assessing PCL Balance
-
Remove all deforming osteophytes.
-
Perform required soft tissue releases.
-
Align femoral component properly.
-
Match bone resection to implant thickness in:
-
Extension.
-
Flexion.
-
Assessing PCL Balance
The “Pull-Off” Test
-
At 90° flexion:
-
If tibial trial can be pulled anteriorly ? Flexion gap too loose.
-
The “Lift-Off” (Nutcracker) Sign
-
If tibia lifts anteriorly during flexion:
-
PCL too tight.
-
Posterior rollback restricted.
-
Managing a Tight PCL
Preferred method:
-
Femoral-side release (rather than tibial side).
-
Controlled release in intercondylar notch.
-
Gradual balancing under direct visualization.
Alternative:
-
Tibial bone island preservation technique.
-
Maintain central bone island with PCL insertion.
-
Carefully cut surrounding tibial bone.
-
When to Sacrifice the PCL
-
Persistent instability.
-
Excessive rollback.
-
Uncorrectable imbalance.
-
Restricted motion despite balancing.
Not dogmatic:
-
Convert to PS if balance cannot be achieved.
-
Approximately 1 in 10 may require sacrifice.
Technical Pearls for PCL Preservation
-
Use specialized retractor with dual prongs:
-
Protects PCL during tibial cut.
-
-
Avoid central posterior saw penetration.
-
Lift osteotomized bone from medial and lateral sides.
-
Use meniscal grasper to control tibial cut segment.
-
Carefully outline and preserve PCL insertion during tibial resection.
Clinical Evidence
Studies suggest:
-
Greater knee extensor moment during stair climbing in CR knees.
-
Lower medial compartment loading compared to PS.
-
Comparable or favorable long-term survivorship.
Personal Clinical Experience
-
4,000 primary CR knees over several years.
-
Very low conversion rate to PS.
-
No major CR-specific complications observed.
-
Successful use even in severe deformities.
Common Misconception
CR knees are often considered:
-
More technically demanding.
-
Less forgiving.
Experience suggests:
-
If surgeon can perform PS reliably, CR is equally manageable.
-
Proper technique and balancing are key.
Summary Points
-
Cruciate-retaining TKA provides outcomes comparable to PS designs.
-
Bone preservation is a significant surgical advantage.
-
PCL need not be pristine to be retained.
-
Proper assessment and balancing are essential.
-
Conversion to PS should remain an option when required.


Leave a Reply