Courtesy: Prof Hitesh Shah, Professor of Paediatric Orthopaedics, KMC Manipal, India
Coxa Vara in Children
Introduction
Coxa vara is a pediatric hip deformity characterized by a decreased femoral neck-shaft angle.
The condition alters:
- Hip biomechanics
- Abductor function
- Limb alignment
If progressive, it can lead to gait abnormalities, limb shortening, and long-term hip dysfunction.
Normal Femoral Alignment
The femoral neck-shaft angle changes with age.
At Birth
- Approximately 150°
At Skeletal Maturity
- Approximately 125°
Because the angle changes during growth, assessment must always be:
- Age-based
Definition
Coxa vara is defined as:
- Femoral neck-shaft angle less than 2 standard deviations below the normal mean for age
Etiology
Congenital Causes
Important congenital causes include:
- Proximal femoral focal deficiency (PFFD)
Developmental Coxa Vara
A common pediatric form characterized by:
- Progressive deformity during growth
Acquired Causes
Other causes include:
- Post-infective deformity
- Post-traumatic deformity
- Fibrous dysplasia
- Metabolic bone disease
- Osteogenesis Imperfecta
- Legg-Calvé-Perthes disease
- Slipped Capital Femoral Epiphysis
Pathophysiology
Varus deformity of the proximal femur leads to:
- Increased shear forces across the femoral neck
- Progressive deformity
- Weakening of hip abductors
- Limb shortening
This contributes to gait abnormalities and mechanical dysfunction.
Clinical Features
Common Symptoms
Patients may present with:
- Limp
- Hip pain
- Fatigue during walking
- Limb shortening
Gait Abnormalities
Typical gait findings include:
- Trendelenburg gait
- Abductor weakness
Important Clinical Sign
A classic examination finding is:
- Adduction greater than abduction
This is an important diagnostic clue.
Radiographic Evaluation
Standard Imaging
Radiographic evaluation usually includes:
- AP pelvis radiograph
- Frog-leg lateral view
- Long-leg alignment radiographs
Important Measurements
Neck-Shaft Angle
Determines severity of varus deformity.
Hilgenreiner Epiphyseal (HE) Angle
The HE angle is a key parameter used to guide management.
Interpretation
Less Than 25°
- Usually considered normal
25–45°
- Observation may be appropriate
Greater Than 60°
- Surgical correction is generally recommended
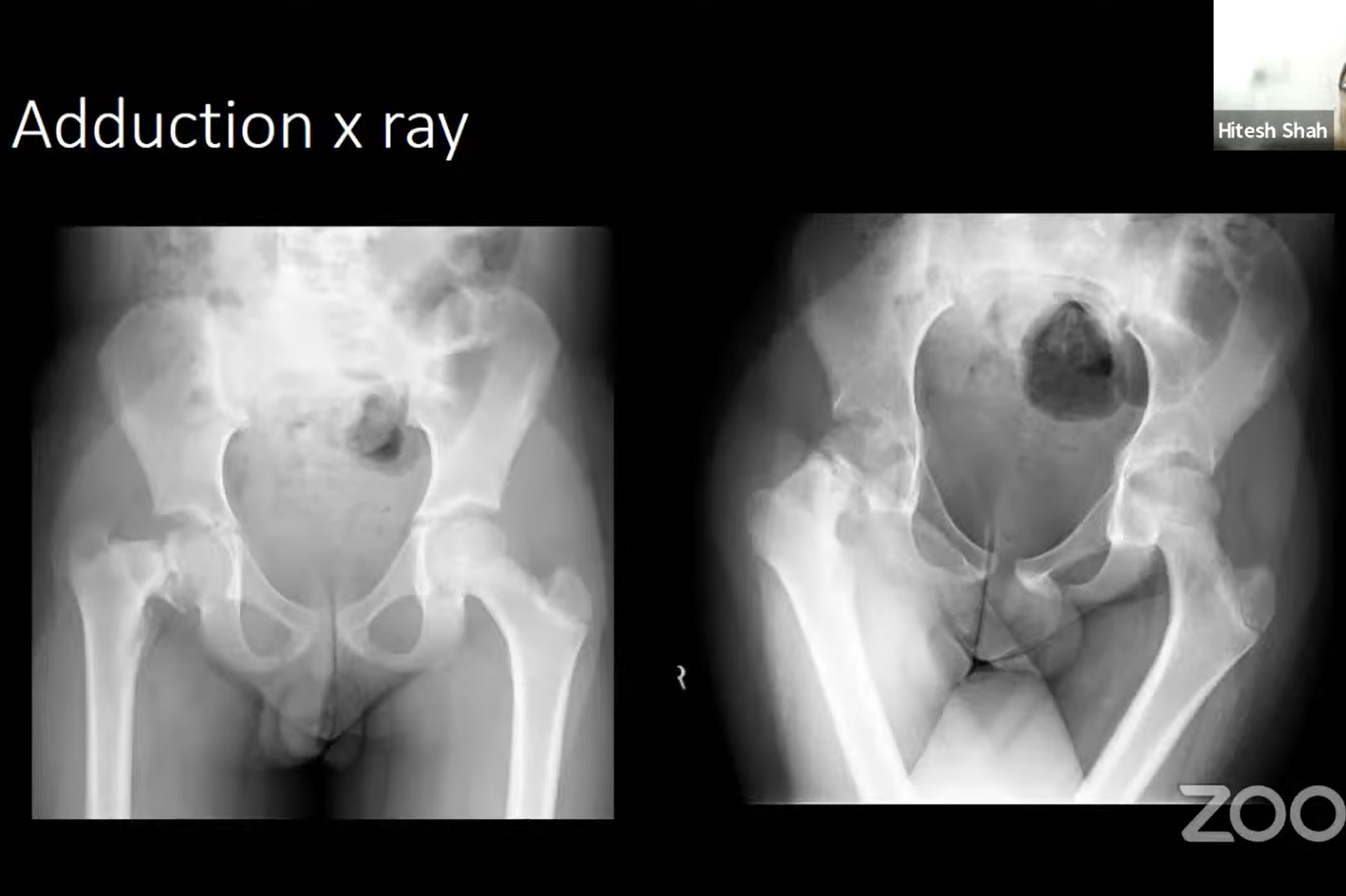
Adduction Radiograph
An adduction view helps assess:
- Potential correction
- Femoral head coverage
- Reducibility of deformity
This is useful for surgical planning.
Types of Coxa Vara
Major categories include:
- Congenital coxa vara
- Developmental coxa vara
- Acquired coxa vara
Management depends on underlying cause and progression.
Management
Observation
Observation may be appropriate for:
- Mild deformity
- Non-progressive cases
- Low HE angle
Regular follow-up is important.
Valgus Osteotomy
Main Surgical Treatment
Valgus-producing proximal femoral osteotomy is the primary surgical treatment.
Goals of Surgery
The procedure aims to:
- Correct varus deformity
- Reduce shear forces
- Improve hip biomechanics
- Restore abductor function
Growth Modulation
Growth-guiding procedures may be considered when:
- Physeal abnormalities contribute to deformity
Trochanteric Epiphysiodesis
Indications
Performed in younger children, typically:
- Before 8–9 years of age
Purpose
Helps prevent:
- Greater trochanter overgrowth
- Progressive abductor dysfunction
Trochanteric Transfer
May be required in selected patients to:
- Improve abductor mechanics
- Reduce impingement
Neck Lengthening Procedures
Neck lengthening may be:
- Relative
- Absolute
depending on deformity severity and anatomy.
Special Situations
Post-Traumatic Coxa Vara
Management focuses on:
- Correction of deformity
- Treatment of non-union if present
Osteopenic Bone
Patients with poor bone quality may require:
- Intramedullary fixation
- Specialized implants
for improved stability.
Complications
Potential complications include:
- Recurrence of deformity
- Growth arrest
- Implant-related complications
- Persistent limp
- Residual limb length discrepancy
Long-term follow-up is essential.
Follow-Up
Patients should be monitored until:
- Skeletal maturity
This helps identify:
- Recurrence
- Progressive deformity
- Growth-related complications
Key Clinical Pearls
- Coxa vara is defined using age-based neck-shaft angle values.
- Developmental coxa vara is a common pediatric form.
- Adduction greater than abduction is a classic clinical sign.
- HE angle is critical for treatment planning.
- Valgus osteotomy is the primary surgical treatment.
- Trochanteric overgrowth can worsen abductor dysfunction.
- Long-term follow-up until skeletal maturity is essential.
Final Take-Home Message
Coxa vara in children is a proximal femoral deformity characterized by decreased neck-shaft angle and altered hip mechanics.
The condition may be congenital, developmental, or acquired, and careful evaluation of the underlying cause is essential.
Management depends on:
- Severity
- Progression
- HE angle
- Functional impairment
Valgus osteotomy remains the cornerstone of treatment for progressive deformity, while long-term surveillance is necessary to monitor growth and prevent recurrence.

Leave a Reply