Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
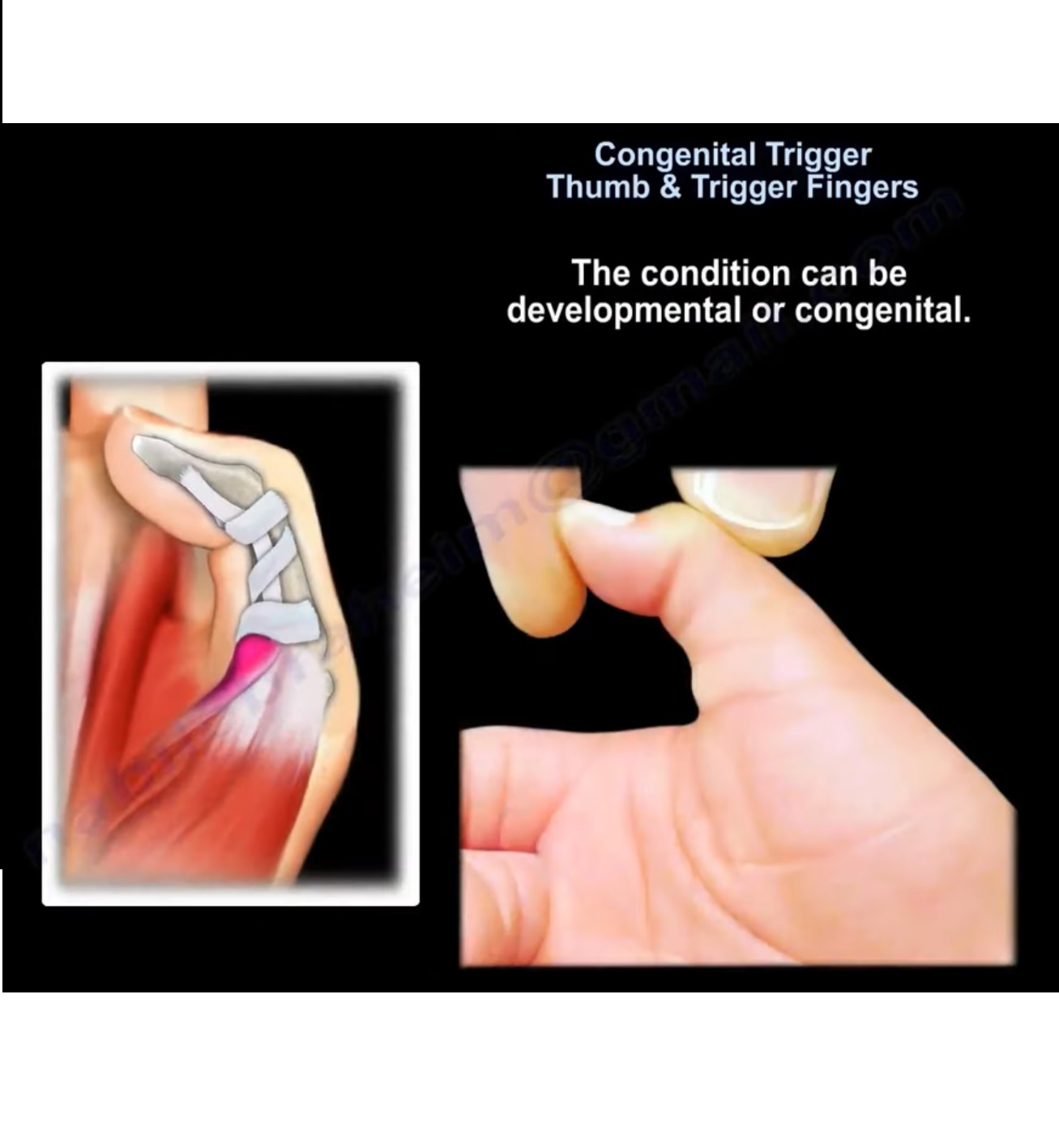
Congenital Trigger Thumb and Trigger Fingers in Children
Introduction
Congenital trigger thumb is a pediatric hand condition characterized by:
- Flexion deformity of the thumb
- Triggering during motion
- Inability to fully extend the interphalangeal (IP) joint
Although commonly called “congenital,” many cases are actually developmental and become noticeable during infancy or early childhood.
Trigger thumb is significantly more common than pediatric trigger fingers.
Congenital Trigger Thumb
Definition
Congenital trigger thumb is a condition involving:
- Flexion deformity at the thumb IP joint
- Impaired gliding of the flexor pollicis longus tendon
The deformity may be:
- Intermittent
- Fixed
depending on disease progression.
Epidemiology
Important points include:
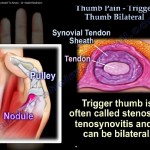
- Approximately 25% of cases are bilateral
- Usually presents in early childhood
- More common than trigger fingers in children
Pathophysiology
Tendon-Pulley Mismatch
The primary abnormality involves:
- Thickening of the flexor pollicis longus (FPL) tendon
The tendon becomes larger than the:
- A1 pulley
This causes:
- Impaired tendon gliding
- Triggering
- Progressive flexion contracture
Notta’s Node
A characteristic finding is:
- Notta’s node
This is a palpable nodule located near the:
- Metacarpophalangeal (MCP) joint
and represents thickening of the FPL tendon.
Clinical Features
Typical Presentation
Common findings include:
- Flexed IP joint of the thumb
- Inability to actively extend the thumb
- Palpable nodule at the base of the thumb
- Triggering or locking
Examination Findings
The thumb may:
- Click during motion
- Lock in flexion
- Become fixed in longstanding cases
Imaging
Radiographs
X-rays are typically:
- Normal
Imaging is mainly useful to exclude alternative diagnoses if presentation is atypical.
Natural History
Spontaneous Resolution
Some cases improve spontaneously in infancy.
However:
- Spontaneous correction becomes unlikely after approximately 2 years of age
Persistent deformity beyond this age often requires surgery.
Management
Conservative Treatment
Indications
Conservative management is usually attempted in:
- Infants younger than 1 year
Non-Operative Measures
Treatment options include:
- Observation
- Passive stretching exercises
- Extension splinting
Outcomes
Approximately:
- 50% of infants may improve without surgery
Indications for Surgery
Surgery is recommended when there is:
- Failure of conservative treatment
- Persistent fixed deformity after 1 year
- No spontaneous correction
Surgical Treatment
A1 Pulley Release
The standard surgical procedure is:
- Release of the A1 pulley
This restores smooth tendon gliding.
Important Surgical Precautions
Radial Digital Nerve Protection
Careful dissection is essential to protect the:
- Radial digital nerve
Oblique Pulley Preservation
The oblique pulley should not be released because this may cause:
- Bowstringing of the tendon
Outcomes
Surgical release generally provides:
- Excellent correction
- Restoration of thumb motion
- Low recurrence rate
Trigger Fingers in Children
Overview
Pediatric trigger fingers differ significantly from adult trigger fingers.
Important differences include:
- Often involves multiple fingers
- Triggering occurs more distally
Pathophysiology
Unlike adult trigger finger, pediatric trigger fingers are commonly caused by:
- Flexor digitorum profundus (FDP) tendon triggering
at the level of the:
- A2 pulley
rather than the A1 pulley.
Clinical Features
Patients may present with:
- Finger triggering
- Locking
- Difficulty with flexion and extension
- Multiple digit involvement
Management
Surgical Treatment
The commonly performed procedure is:
- Excision of one slip of the flexor digitorum superficialis (FDS)
Goal of Surgery
The aim is to:
- Improve tendon gliding
- Eliminate triggering
Complications
Potential complications include:
- Incomplete release
- Recurrence
- Digital nerve injury
- Bowstringing if pulley preservation is inadequate
Careful surgical technique minimizes risk.
Key Clinical Pearls
- Trigger thumb is more common than trigger finger in children.
- Notta’s node is a classic finding in trigger thumb.
- The deformity is caused by mismatch between the FPL tendon and A1 pulley.
- Spontaneous resolution becomes less likely after 2 years of age.
- A1 pulley release is the standard surgical treatment.
- In pediatric trigger fingers, pathology is commonly at the A2 pulley.
- Preservation of the oblique pulley is essential to avoid bowstringing.
Final Take-Home Message
Congenital trigger thumb is a common pediatric hand condition characterized by flexion deformity of the thumb due to impaired tendon gliding at the A1 pulley.
Early conservative treatment may help in infants, but persistent deformity often requires surgical release.
Pediatric trigger fingers differ from adult trigger fingers in both pathophysiology and treatment, requiring careful evaluation and specialized management.

Leave a Reply