Courtesy: Mr Michael Uglow FRCSOrth, Paley’s Orthopaedic Institute, UAE
Congenital Pseudarthrosis of the Tibia (CPT)
Introduction
Congenital pseudarthrosis of the tibia (CPT) is a rare pediatric condition characterized by:
- Anterolateral bowing of the tibia
- Progressive weakening of bone
- Pathological fracture
- Failure of fracture healing leading to pseudarthrosis
The condition is challenging because it involves both:
- Biological failure of bone healing
- Mechanical instability
Association with Neurofibromatosis
A strong association exists between CPT and Neurofibromatosis Type 1.
Patients should therefore be evaluated for:
- Café-au-lait spots
- Neurofibromas
- Other manifestations of NF1
Pathophysiology
Biological Abnormality
The normal bone healing process is replaced by:
- Fibrous hamartomatous tissue
This tissue inhibits:
- Osteogenesis
- Normal union
while increasing:
- Bone resorption
Bone Quality
Approximately 30% of patients demonstrate:
- Osteopenia
which further compromises healing potential.
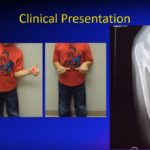
Clinical Features
Typical Presentation
Common findings include:
- Anterolateral bowing of the tibia
- Progressive deformity
- Pathological fracture
- Persistent non-union
The deformity usually presents in early childhood.
Classification
Paley Classification
Type 1
- Tibial deformity without fracture
Important Principle
Surgery should generally be avoided if fracture has not occurred.
Type 2
- Associated fibular fracture
Type 3
- Tibial fracture with pseudarthrosis
Type 4
- Fracture involving both tibia and fibula
Type C
- Presence of bone defect
Fundamental Treatment Principles
Successful treatment requires:
- Stable mechanical fixation
- Complete excision of fibrous hamartoma
- Promotion of bone healing
- Prevention of refracture
Historical Treatment Methods
Intramedullary Rod Fixation
Historically used but associated with:
- High refracture rates
Ilizarov External Fixation
Advantages:
- Gradual correction
- Compression and stabilization
Limitations:
- Multiple procedures
- Prolonged treatment duration
Vascularized Fibular Grafting
Provided moderate success but outcomes were variable.
Biological Adjuvants
BMP and Bisphosphonates
Bone morphogenetic protein (BMP) and bisphosphonates have improved healing rates, although results remain inconsistent when used alone.
Modern Standard Treatment: Cross-Union Technique
Concept
The modern preferred treatment is the:
- Tibia-fibula cross-union technique
This creates a robust union between the tibia and fibula, improving:
- Stability
- Healing potential
- Resistance to refracture
Advantages
Cross-union significantly reduces:
- Refracture risk
and provides superior long-term mechanical stability.
Prevention Strategies
Early Bracing
Protective bracing may help:
- Prevent fracture
- Reduce progression of deformity
Guided Growth
May be useful in selected patients to control progressive deformity.
Surgical Technique
Key Surgical Steps
Modern surgical management typically includes:
- Excision of fibrous hamartoma
- Freshening of bone ends
- Intramedullary fixation
- Fibular stabilization
- Plate fixation
- Bone grafting
- Biological augmentation
Important Technical Details
Internal Fixation
Fixation may include:
- Intramedullary nail
- Fibular wire
- Medial plate fixation
Bone Grafting
Bone grafting is commonly combined with:
- BMP
- Periosteal grafting
to stimulate osteogenesis.
Interosseous Membrane
Removal of the interosseous membrane facilitates:
- Tibia-fibula cross-union formation
Postoperative Management
Bisphosphonate Therapy
Postoperative bisphosphonates may improve:
- Bone density
- Healing quality
Growth Monitoring
Long-term follow-up is essential to monitor:
- Limb alignment
- Growth disturbance
- Implant position
- Recurrence
Outcomes
Modern cross-union techniques have demonstrated:
- Near 100% union rates
- Low refracture rates
These results are substantially better than historical methods.
Implant Considerations
Plate Position
Plates are commonly placed:
- Medially
to improve fixation and reduce soft tissue irritation.
Implant Removal
Implants may require later removal if complications occur.
Complications
Potential complications include:
- Implant migration
- Skin irritation or breakdown
- Refracture
- Residual deformity
- Limb length discrepancy
Careful long-term surveillance is necessary.
Key Clinical Pearls
- CPT is both a biological and mechanical problem.
- Strong association exists with Neurofibromatosis Type 1.
- Anterolateral bowing is the classic deformity.
- Avoid surgery in patients without fracture whenever possible.
- Cross-union technique is currently considered the gold standard.
- Stable fixation and biological enhancement are essential.
- Early prevention and bracing may reduce fracture risk.
Final Take-Home Message
Congenital pseudarthrosis of the tibia is a rare but difficult pediatric condition characterized by pathological fracture and persistent non-union.
Traditional treatments had high failure and refracture rates, but modern tibia-fibula cross-union techniques have dramatically improved outcomes.
Successful treatment depends on:
- Stable mechanical fixation
- Complete biological optimization
- Long-term follow-up
- Prevention of refracture and deformity progression

Leave a Reply