COurtesy: William Mackenzie, Jefferson Medical College, USA
OVERVIEW
-
Congenital femoral deficiency is a spectrum of congenital anomalies involving deficiency, deformity, and instability of the femur.
-
Severity ranges from mild femoral shortening to near-complete absence of the femur.
-
Limb length discrepancy, joint instability, and associated deformities are common.
-
Management is individualized and depends on predicted limb length discrepancy and joint stability.
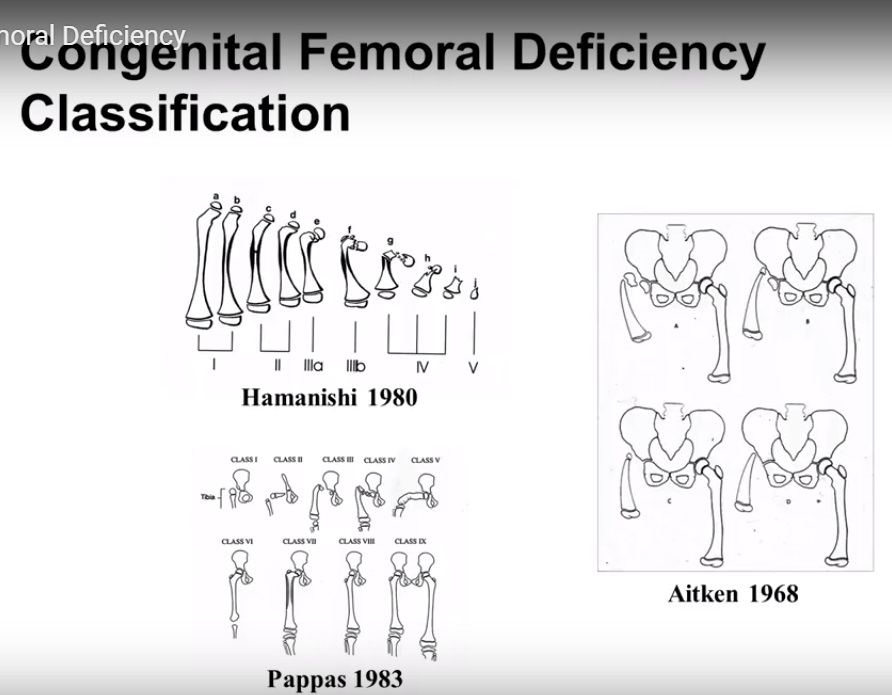
CLASSIFICATIONS
Several classification systems have been described:
-
Aitken classification (1968)
-
Hamanishi classification (1980)
-
Pappas classification (1983)
-
Gillespie classification (1998)
-
Paley classification (reconstruction-oriented)
GILLESPIE TYPE A / PALEY TYPE 1A (MILD FORM)
Etiology
-
Etiology is unknown.
-
No established genetic predisposition.
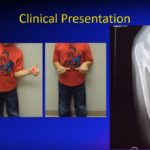
Clinical Features
-
Limb length discrepancy approximately 20 to 30 percent.
-
Foot level at mid tibia or below.
-
Short thigh segment.
-
Anterolateral bowing of the femur.
-
Hip flexion contracture.
-
Femoral retroversion.
-
Genu valgum.
Associated Findings
-
Acetabular dysplasia.
-
Coxa vara, usually non-progressive.
-
Cruciate ligament deficiency.
-
Lateral patellar instability.
-
Fibular hemimelia.
Management
Management depends on predicted limb length discrepancy at skeletal maturity:
-
Shoe lift for mild discrepancy.
-
Epiphysiodesis for moderate discrepancy.
-
Reconstruction for discrepancy greater than 4 to 5 centimeters:
-
Periacetabular osteotomy.
-
Proximal femoral osteotomy.
-
Femoral lengthening.
-
Distal femoral realignment.
-
Principles of Femoral Lengthening
-
Femoral lengthening is technically demanding.
-
Avoid excessive lengthening in a single stage.
-
Soft tissue releases should be considered.
-
High risk of posterolateral knee subluxation.
-
Fractures are common.
Prevention of Joint Instability
-
Structured physical therapy.
-
Maintenance of knee extension.
-
Primary and secondary soft tissue releases.
-
Extension of external fixation across the joint when required.
-
Joint reconstruction when indicated.
-
Lengthening of adjacent stable segments.
-
Avoid over-lengthening.
GILLESPIE TYPE B AND C / PALEY TYPE 1B OR 2A
Etiology
-
Unknown etiology.
-
No genetic predisposition.
Clinical Features
-
Limb length discrepancy approximately 30 to 50 percent.
-
Foot positioned above the level of the proximal tibia.
-
Short and broad thigh segment.
-
Hip and knee flexion contractures.
-
External rotation deformity of the limb.
Associated Findings
-
Fibular hemimelia (50 to 80 percent).
-
Cruciate ligament deficient knee.
-
Foot deformities.
-
Congenital spinal anomalies.
-
Congenital heart disease.
Management Considerations
Decision-making depends on:
-
Predicted limb length discrepancy at maturity.
-
Hip stability.
-
Adequacy of musculature.
-
Presence of hip dysplasia.
-
Limb malrotation.
-
Foot and ankle function.
Treatment Options
Predicted Limb Length Discrepancy Less Than 50 Percent of the Opposite Femur
With a stable hip and functional foot (more than 3 rays):
-
Staged limb lengthening and realignment.
-
Epiphysiodesis as an adjunct.
Predicted Limb Length Discrepancy Greater Than 15 to 20 Centimeters
Or unstable hip or non-functional foot (less than 2 rays):
-
Limb lengthening is contraindicated.
-
Management options include:
-
Prosthetic fitting.
-
Amputation (Boyd or Syme procedure), with or without knee arthrodesis.
-
Rotationplasty.
-
Iliofemoral fusion.
-
Bilateral Congenital Femoral Deficiency
-
Avoid procedures that compromise overall function.
-
Emphasis is on symmetry and functional mobility rather than length equalization.
PALEY CLASSIFICATION OF CONGENITAL FEMORAL DEFICIENCY
Children with congenital femoral deficiency demonstrate a spectrum of femoral deficiency, deformity, and joint instability. Earlier classifications were oriented toward amputation and prosthetic management. Dror Paley introduced a classification system focused on reconstructive limb lengthening strategies.
Type 1: Intact Femur With Mobile Hip and Knee
-
Type 1A: Normal ossification of proximal femur.
-
Type 1B: Delayed ossification of proximal femur:
-
Neck
-
Subtrochanteric
-
Combined neck and subtrochanteric.
-
Type 2: Mobile Pseudoarthrosis
Greater trochanteric apophysis present; knee usually mobile.
-
Type 2A: Femoral head mobile within acetabulum.
-
Type 2B: Femoral head partially fused to acetabulum.
-
Type 2C: Femoral head and acetabulum completely fused or absent.
Type 3: Diaphyseal Deficiency of Femur
Greater trochanteric apophysis absent.
-
Type 3A: Distal physis present, knee motion greater than 45 degrees.
-
Type 3B: Distal physis present, knee motion less than 45 degrees.
-
Type 3C: Complete distal femoral deficiency or fusion of distal femur to tibia.
Type 4: Distal Femoral Deficiency
-
Proximal femur is relatively normal.
-
Distal femur is deficient.
SUPERHIP PROCEDURE
The SUPERhip procedure was developed by Dror Paley in 1997.
SUPER stands for Systematic Utilitarian Procedure for Extremity Reconstruction.
-
Designed to address severe hip deformities in congenital femoral deficiency.
-
Can be performed as early as 2 years of age.
-
Ideally performed between 2 and 3 years.
-
Can also be performed in older children and adults.
Components of SUPERhip
1. Soft Tissue Releases
-
Correct hip flexion, abduction, and external rotation contractures.
-
Restores functional hip motion.
2. Femoral Osteotomy
-
Corrects proximal femoral varus, flexion, and external rotation deformities.
-
Restores mechanical alignment.
3. Pelvic Osteotomy
-
Improves femoral head coverage.
-
Corrects acetabular dysplasia.
SUPERKNEE PROCEDURE
The SUPERknee procedure, developed in 1994, addresses knee instability associated with congenital femoral deficiency.
Objectives
-
Reconstruction of anterior cruciate ligament and posterior cruciate ligament.
-
Realignment of the patella.
-
Correction of knee flexion contracture.
Surgical Principles
-
Fascia lata is used to reconstruct both cruciate ligaments.
-
Fascia lata is divided into two components:
-
FL1 for anterior cruciate ligament reconstruction.
-
FL2 for posterior cruciate ligament reconstruction.
-
-
FL1 is passed beneath the lateral collateral ligament and through the intercondylar notch.
-
FL2 is passed through the intermuscular septum and sutured to itself.
-
Both ligaments are interconnected for reinforcement.
-
The reconstructed posterior cruciate ligament is often referred to as Paley ligament.
Customization
-
Each SUPERknee procedure is individualized.
-
Components are performed based on the patient’s specific instability and deformity pattern.
-
May be performed independently or in combination with SUPERhip.
KEY PRINCIPLES
-
Accurate classification guides treatment.
-
Joint stability is more important than limb length alone.
-
Over-lengthening increases complications.
-
Reconstruction requires staged planning and long-term follow-up.
-
Functional outcome takes precedence over cosmetic symmetry.


Leave a Reply