Courtesy: Dr Nijil Vasukutty, FRCS Orth, UK
Overview
Midfoot trauma includes injuries involving:
- Chopart joint complex
- Lisfranc joint complex
- Navicular
- Cuboid
- Cuneiform bones
- Surrounding ligaments
These injuries may occur following:
- Low energy twisting injuries
- Sports injuries
- Road traffic accidents
- Crush injuries
A significant number of midfoot injuries are subtle and easily missed during the initial assessment.
Midfoot Anatomy
Midfoot Bones
The midfoot consists of:
- Navicular
- Cuboid
- Medial cuneiform
- Intermediate cuneiform
- Lateral cuneiform
Functional Columns of the Foot
Medial Column
Includes:
- Talus
- Navicular
- Three cuneiforms
- First metatarsal
- Second metatarsal
- Third metatarsal
Functions:
- Stability
- Weight transmission
Lateral Column
Includes:
- Cuboid
- Fourth metatarsal
- Fifth metatarsal
- Anterior process of calcaneus
Functions:
- Flexibility
- Adaptation to uneven ground
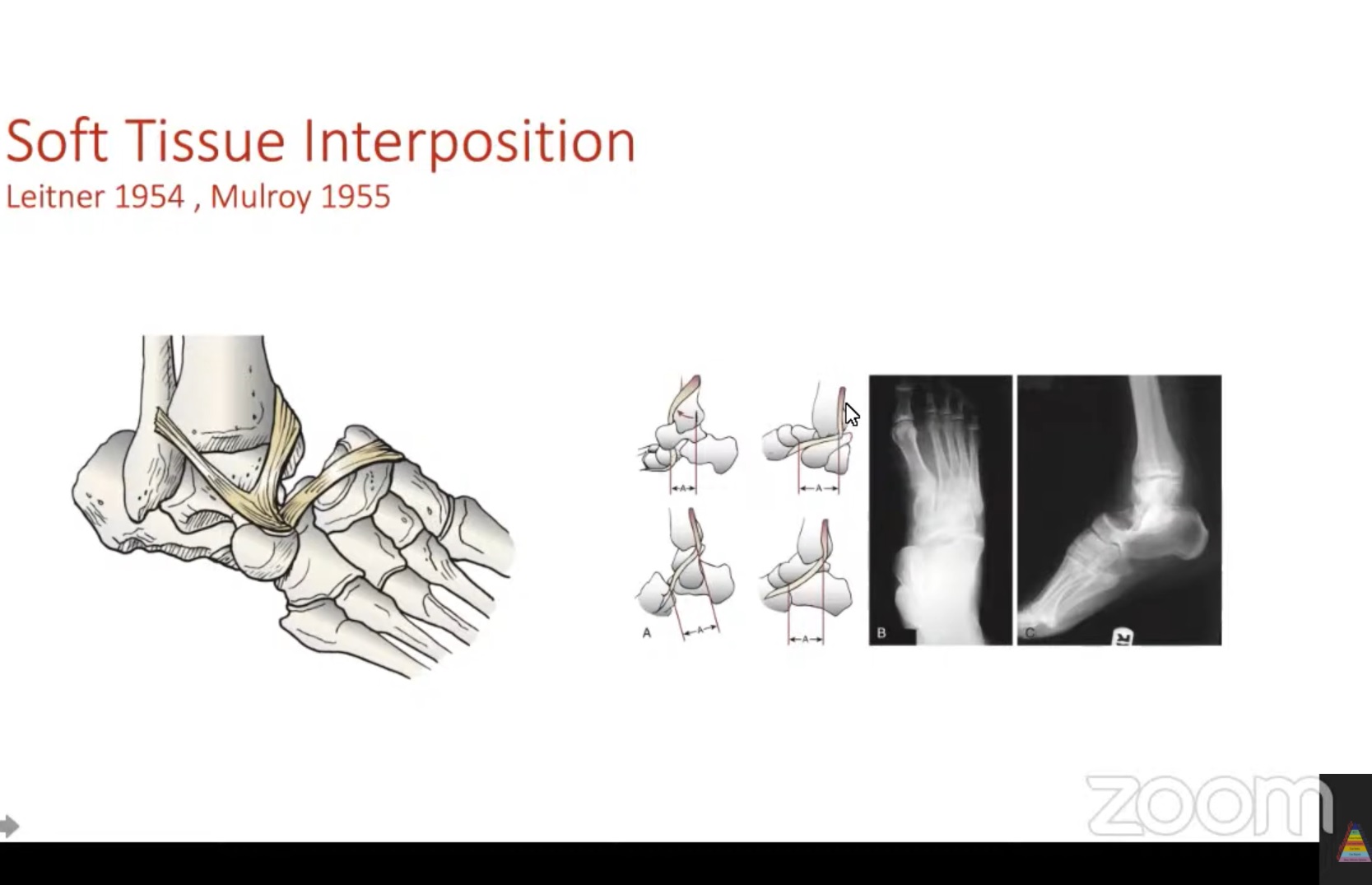
Important Ligaments
Key stabilizers include:
- Dorsal calcaneocuboid ligament
- Bifurcate ligament
- Dorsal talonavicular ligament
- Plantar calcaneonavicular (spring) ligament
Chopart Joint Injuries
Components of the Chopart Joint
The Chopart joint consists of:
Talonavicular Joint
Calcaneocuboid Joint
These joints provide mobility while maintaining midfoot stability.
Mechanisms of Injury
- Abduction injuries
- Adduction injuries
- Axial loading
- Direct trauma
- Crush injuries
Clinical Pearl
Even small fractures of the:
- Cuboid
- Navicular
may indicate significant associated ligament disruption.
Clinical Presentation
Patients commonly present with:
- Midfoot pain
- Swelling
- Local tenderness
- Difficulty bearing weight
- Deformity in severe injuries
Important Clinical Sign
Plantar Midfoot Ecchymosis
- Suggests plantar ligament disruption
- Strongly indicates midfoot instability
- Should raise suspicion for Lisfranc injury
Imaging Evaluation
Plain Radiographs
Obtain:
- AP view
- Lateral view
- Oblique view
Weight Bearing Radiographs
Very important because they can demonstrate:
- Subtle instability
- Loss of alignment
- Joint widening
that may not be visible on standard non weight bearing films.
CT Scan
Useful for:
- Fracture characterization
- Joint congruity assessment
- Preoperative planning
MRI
Indications:
- Suspected ligament injury
- Persistent symptoms with normal radiographs
- Assessment of soft tissue damage
Principles of Treatment
Management depends on:
- Fracture displacement
- Joint congruity
- Ligament stability
- Soft tissue condition
Non Surgical Treatment
Indications
- Stable ligament injuries
- Small avulsion fractures
- Undisplaced fractures
- No evidence of instability
Treatment
- Cast or walking boot
- Protected weight bearing
- Gradual rehabilitation
Surgical Treatment
Indications
- Displaced fractures
- Fracture dislocations
- Unstable ligament injuries
- Loss of foot alignment
Goals of Surgery
- Restore anatomy
- Preserve foot length
- Restore column alignment
- Achieve stable fixation
- Protect soft tissues
Temporary Stabilization
In severe trauma, definitive surgery is often delayed until swelling improves.
Temporary options include:
- Closed reduction
- K wire transfixation
- External fixation
Fixation Methods
Common implants include:
- Cannulated screws
- Locking plates
- Bridge plates
- Kirschner wires
The objective is anatomical reduction and stable fixation.
Postoperative Care
Typical protocol:
First 6 to 8 Weeks
- Strict non weight bearing
Thereafter
- Walking boot
- Progressive weight bearing
- Physiotherapy
Additional Considerations
- DVT prophylaxis when indicated
- Monitoring for wound complications
Lisfranc Injuries
Anatomy
The Lisfranc complex consists of the tarsometatarsal joints.
Key Structure
The second tarsometatarsal joint acts as the keystone of the midfoot and is the primary stabilizing structure.
Mechanisms
- Twisting injuries
- Axial loading
- Direct trauma
- High energy injuries
Clinical Features
- Midfoot pain
- Swelling
- Difficulty weight bearing
- Plantar ecchymosis
Imaging Findings
Characteristic Sign
Increased distance between:
- First metatarsal
- Second metatarsal
suggesting Lisfranc ligament disruption.
Treatment of Lisfranc Injuries
Stable Injuries
- Immobilization
- Non weight bearing for approximately 6 weeks
Unstable Injuries
Require surgery:
- Open reduction
- Internal fixation with screws or plates
Selected Cases
Primary fusion may be considered.
Open and Crush Injuries
These represent severe limb threatening injuries.
Initial Priorities
- ATLS principles
- Neurovascular assessment
- Reduction of dislocations
- Appropriate imaging
Infection Prevention
May require:
- Repeated debridement
- Intravenous antibiotics
- Temporary stabilization
Limb Salvage Considerations
Factors favouring amputation rather than salvage may include:
- Major vascular injury
- Extensive soft tissue loss
- Irreparable nerve injury
- Severe destruction of midfoot architecture
Decision making should involve a multidisciplinary team.
Prognosis
Better outcomes are associated with:
- Early diagnosis
- Anatomical reduction
- Stable fixation
- Appropriate rehabilitation
Recovery Timeline
- Pain and swelling may persist for months
- Return to sports often requires 6 to 12 months
- Some patients develop post traumatic arthritis despite optimal treatment
Key Clinical Pearls
- Midfoot injuries are commonly missed.
- Plantar ecchymosis is an important sign of instability.
- Weight bearing radiographs are essential when possible.
- Small cuboid or navicular fractures may indicate major ligament injury.
- CT scanning is invaluable for fracture assessment and operative planning.
- Accurate restoration of foot column length and alignment is critical.
- Anatomical reduction is the most important predictor of a good outcome.
- Complex midfoot injuries often require staged treatment and prolonged rehabilitation.

Leave a Reply