Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Definition
-
The muscles of the limbs are organized into closed anatomical compartments.
-
These compartments are bounded by strong, relatively noncompliant fascial membranes.
-
A compartment is defined as a closed space containing muscles, blood vessels, and nerves surrounded by fascia.
-
Compartment syndrome occurs due to elevation of interstitial pressure within a closed osteofascial compartment, leading to microvascular compromise.
-
Compartments with rigid fascial or osseous boundaries are most commonly involved, such as:
-
Anterior and deep posterior compartments of the leg
-
Volar compartment of the forearm
-
Types of Compartment Syndrome
Based on the cause and duration of increased pressure:
-
Acute compartment syndrome (surgical emergency)
-
Chronic exertional compartment syndrome
Anatomy of Compartments
Upper Limb
Arm
-
Anterior compartment
-
Posterior compartment
Forearm
-
Dorsal compartment
-
Superficial volar compartment
-
Deep volar compartment
-
Mobile wad
Hand
-
Four dorsal interossei
-
Three volar interossei
-
Thenar compartment
-
Hypothenar compartment
-
Adductor compartment
-
Mid-palm compartment
Lower Limb
Thigh
-
Anterior compartment
-
Posterior compartment
-
Medial compartment
Leg
-
Anterior compartment
-
Lateral compartment
-
Superficial posterior compartment
-
Deep posterior compartment
Foot
-
Medial compartment
-
Superficial compartment
-
Lateral compartment
-
Adductor compartment
-
Four interossei compartments
-
Calcaneal compartment
Pathophysiology
-
An insult to local tissue homeostasis leads to:
-
Increased intracompartmental pressure
-
Reduced capillary blood flow
-
Tissue ischemia
-
Cellular hypoxia and necrosis
-
-
The Eaton and Green vicious cycle explains the progressive worsening of ischemia and edema.
Etiology of Acute Compartment Syndrome
1. Decreased Compartment Size
-
Tight bandages, dressings, or casts
-
Burn eschar
-
External compression such as prolonged limb positioning
-
Military anti-shock garments or tourniquets
-
Entrapment under heavy weights
-
Tight closure of fascial defects
-
Excessive traction
-
Limb lengthening procedures
-
Intramedullary nailing in neglected fractures or deformity correction
2. Increased Compartment Content
-
Fractures, both open and closed (most common cause)
-
Crush injuries and blunt trauma
-
Vigorous or prolonged exercise
-
Animal bites and stings
-
Hemorrhage or anticoagulant use
-
Ruptured cysts such as Baker’s cyst
-
Revascularization after ischemia
-
Intravenous fluid extravasation
-
High-pressure injections
-
Intraosseous infusion in children
-
Reaming during intramedullary nailing
-
Use of fluid pumps during arthroscopy
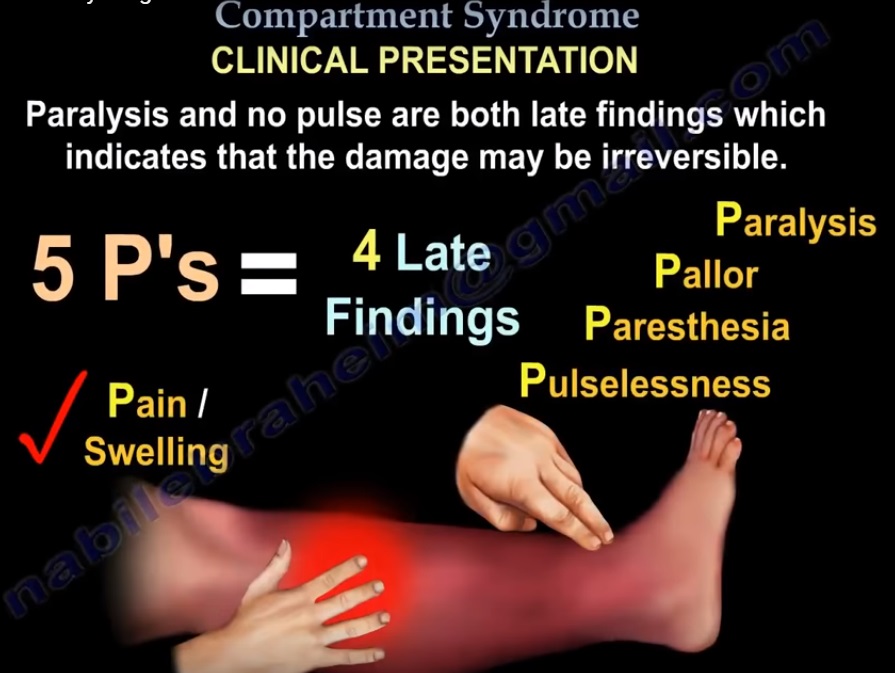
Clinical Evaluation: Characteristic Features
The classic clinical features include:
-
Pain out of proportion to injury
-
Paresthesia or hypoesthesia
-
Pallor
-
Poikilothermia
-
Pulselessness
-
Paralysis
-
A seventh feature is raised intracompartmental pressure
Pain
-
Earliest and most important symptom
-
Severe, deep, burning pain disproportionate to injury
-
Exacerbated by passive stretching of involved muscles
-
Pain may be absent in cases of nerve injury, anesthesia, or heavy analgesia
-
Assessment is difficult in unconscious or sedated patients
Paresthesia
-
Often an early but unreliable symptom
-
In anterior leg compartment syndrome, numbness between the first 2 toes may be the first sign
-
Sensory testing includes:
-
Light touch
-
Pinprick
-
Two-point discrimination
-
-
Decreased light touch sensation is the earliest and most reliable indicator
Paralysis
-
A late finding indicating irreversible muscle and nerve injury
-
Paresis may appear earlier but is difficult to assess due to pain
-
Presence of objective motor deficit indicates advanced disease
Pallor and Pulselessness
-
Rare findings
-
Distal pulses are usually present
-
Suggest associated vascular injury rather than isolated compartment syndrome
Diagnosis
Diagnosis is based on:
-
Clinical history
-
Physical examination
-
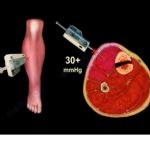
Measurement of intracompartmental pressure when required
-
Intramuscular pH monitoring is rarely used
Important considerations:
-
A single normal pressure reading does not exclude acute compartment syndrome
-
Serial or continuous pressure monitoring is recommended in high-risk cases
Delta Pressure
-
Defined as diastolic blood pressure minus compartment pressure
-
A delta pressure less than 20 to 30 millimeters of mercury indicates need for fasciotomy
Initial Management
-
Remove constrictive dressings or casts
-
Position limb at heart level
-
Avoid limb elevation
-
Correct hypotension and anemia
-
Administer supplemental oxygen
-
Role of mannitol remains unclear
Definitive Management
Non-Operative
-
Appropriate only for impending compartment syndrome
-
Requires close serial clinical and pressure monitoring
Operative Management
Fasciotomy
-
Emergency surgical procedure
-
Relieves compartment pressure
-
Does not reverse existing tissue damage
-
Indicated in:
-
Positive clinical findings
-
Compartment pressure greater than 30 millimeters of mercury
-
Delta pressure less than 20 to 30 millimeters of mercury
-
Progressive clinical deterioration
-
Unconscious or uncooperative patients with elevated pressures
-
Hand compartment pressures greater than 15 to 20 millimeters of mercury
-
Contraindication
-
Missed compartment syndrome beyond 24 to 48 hours due to irreversible damage and high infection risk
Principles of Fasciotomy
-
Early diagnosis
-
Long, extensile incisions
-
Complete release of all involved compartments
-
Preservation of neurovascular structures
-
Debridement of nonviable tissue
-
Timely wound coverage within 7 to 10 days
Postoperative Care and Rehabilitation
-
Leave wounds loosely packed
-
Apply bulky dressing and splint in functional position
-
Gradual wound closure using shoelace technique or negative pressure wound therapy
-
Second-look surgery after 2 to 5 days
-
Early initiation of range-of-motion exercises
-
Skin grafting if required
-
Limb immobilization for 3 to 5 days after grafting
Complications
-
Myonecrosis
-
Nerve injury
-
Volkmann ischemic contracture
-
Reperfusion syndrome
-
Infection
-
Amputation
-
Death
Chronic Exertional Compartment Syndrome
Overview
-
Also known as exertional or recurrent compartment syndrome
-
Common in young athletes and military recruits
-
Most frequently affects the lower limb
Pathophysiology
-
Exercise-induced muscle volume expansion
-
Increased intramuscular pressure
-
Reduced blood flow
-
Ischemic pain and functional impairment
-
Fascial hernia present in 15 to 40 percent of cases
Clinical Features
-
Exercise-induced pain
-
Compartment tenderness
-
Bilateral involvement is common
-
Fascial hernia may be visible
Diagnosis
-
Intracompartmental pressure testing is the diagnostic standard:
-
Resting pressure of 15 millimeters of mercury or more
-
Pressure of 30 millimeters of mercury at 1 minute post-exercise
-
Pressure of 20 millimeters of mercury at 5 minutes post-exercise
-
Pressure greater than 25 millimeters of mercury at 15 minutes is a reliable cutoff
-
Management
Non-Operative
-
Analgesics
-
Activity modification
-
Physical therapy modalities
Operative
-
Single incision fasciotomy
-
Double mini-incision fasciotomy
-
Double incision fasciotomy
Complications of Chronic Compartment Syndrome Surgery
-
Hemorrhage
-
Skin breakdown
-
Sensory changes
-
Recurrence
-
Infection
-
Deep vein thrombosis
-
Vascular or nerve injury
-
Complex regional pain syndrome

Leave a Reply