Definition and Historical Background
-
Scoliosis is defined as an abnormal curvature of the spine in the coronal plane, typically presenting as an “S” or “C” shaped deformity.
-
A spinal curvature greater than 10 degrees, measured using the Cobb method, is considered diagnostic of scoliosis.
-
Hippocrates (460–377 BC) was the first to describe abnormal spinal curvature and introduced the term scoliosis, derived from the Greek word skolios, meaning crooked.
-
Claudius Galen (131–201 AD) classified spinal deformities into scoliosis, kyphosis, and lordosis.
-
The Growing Spine Study Group and the Children Spine Study Group define early onset scoliosis as any spinal deformity presenting before the age of ten years, irrespective of etiology.
-
Adolescent idiopathic scoliosis refers to spinal curvature developing during the adolescent growth spurt, typically between 10 and 18 years of age, without an identifiable cause.
Idiopathic Scoliosis
-
Idiopathic scoliosis has no identifiable causal agent and is not associated with other systemic diseases.
-
According to the Scoliosis Research Society, idiopathic scoliosis is classified into:
-
Infantile idiopathic scoliosis: younger than 3 years
-
Juvenile idiopathic scoliosis: 4 to 10 years
-
Adolescent idiopathic scoliosis: 10 to 18 years
-
-
Severity of curvature:
-
Mild: less than 25 degrees
-
Moderate: 25 to 50 degrees
-
Severe: greater than 50 degrees
-
Epidemiology and Demographics
-
Adolescent idiopathic scoliosis is the most common form of scoliosis.
-
A positive family history is present in a significant proportion of patients.
-
Prevalence is approximately 4 percent of adolescents.
-
Incidence:
-
Curves between 10 and 20 degrees: approximately 3 percent
-
Curves greater than 30 degrees: approximately 0.3 percent
-
-
Gender distribution:
-
Mild curves: male to female ratio of 1:1
-
Curves greater than 30 degrees: female predominance up to 10:1
-
-
Thoracic curves are more common than lumbar curves.
-
The most common pattern is a right-sided thoracic curve.
Pathophysiology
-
The exact etiology remains unknown.
-
Proposed contributing factors include:
-
Genetic predisposition
-
Neurological abnormalities
-
Hormonal and metabolic factors
-
Skeletal growth imbalance
-
Biomechanical influences
-
Environmental and lifestyle factors
-
Clinical Presentation and History
-
Often detected due to cosmetic concerns raised by parents or caregivers.
-
Frequently identified through school screening programs.
-
A scoliometer reading greater than 7 degrees correlates with an approximate 20-degree coronal plane curve.
-
Most patients are asymptomatic, with:
-
No significant back pain
-
No neurological complaints
-
-
Important historical points include:
-
Age at first detection
-
Evidence of progression
-
Perinatal and developmental history
-
Family history
-
Menstrual history in female patients
-
Physical Examination
General Inspection
-
Attention to body symmetry is critical.
-
Common findings include:
-
Uneven shoulders
-
Prominence of one scapula
-
Lateral deviation of the spine
-
Rib prominence on one side
-
Unequal hip levels
-
Asymmetric waistline
-
Head not centered over the pelvis
-
-
Look for:
-
Café-au-lait spots or skin nevi, suggesting neurocutaneous disorders
-
Foot deformities such as cavovarus feet, which may indicate neural axis abnormalities and require magnetic resonance imaging
-
-
Serial height measurements help identify peak height velocity, which correlates with curve progression.
-
Limb length discrepancy should be excluded, as it can cause compensatory scoliosis.
Spine Examination
-
Inspect for midline skin abnormalities such as hairy patches or dimples, suggestive of spinal dysraphism.
-
Assess for rib rotational deformity.
-
Adams forward bending test is the most important clinical screening test:
-
The patient bends forward while the examiner observes for rib or lumbar prominence.
-
Trunk asymmetry indicates a structural curve.
-
A scoliometer angle less than 7 degrees is considered normal.
-
-
Forward bending in the sitting position helps eliminate limb length inequality.
Neurological Examination
-
Motor strength and sensory testing of upper and lower limbs
-
Deep tendon reflexes
-
Assessment for abnormal abdominal reflexes, clonus, Hoffmann sign, and Babinski sign
-
Gait analysis and evaluation of developmental milestones
Curve Progression
-
Major risk factors for progression include:
-
Initial curve magnitude
-
Curve pattern
-
Remaining skeletal growth
-
Skeletal Maturity Assessment
-
Tanner staging
-
Risser staging based on iliac apophyseal ossification:
-
Risser stage zero indicates significant growth remaining
-
Higher stages indicate reduced growth potential
-
-
After skeletal maturity:
-
Thoracic curves greater than 50 degrees progress by 1 to 2 degrees per year
-
Lumbar curves greater than 40 degrees progress at a similar rate
-
Imaging
Plain Radiographs
-
Standing posteroanterior and lateral views are recommended.
-
Radiographs should include:
-
Cervical spine proximally
-
Iliac crests distally
-
-
Supine side-bending views are used for preoperative planning.
-
Key radiographic parameters assessed:
-
End vertebrae
-
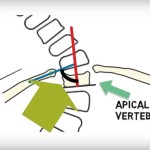
Apical vertebra
-
Stable and neutral vertebrae
-
Curve location and direction
-
Curve magnitude
-
Risser sign
-
Measurement Techniques
-
Cobb angle:
-
A curve greater than 10 degrees defines scoliosis
-
Interobserver and intraobserver error is approximately 3 to 5 degrees
-
-
Coronal balance is assessed using the relationship between the cervical spine plumb line and the central sacral vertical line.
-
Sagittal balance is evaluated from the cervical spine to the sacrum.
-
Clavicle angle is a strong predictor of postoperative shoulder balance.
Vertebral Rotation
-
Nash–Moe method is used to estimate vertebral rotation based on pedicle position.
-
Provides a rough approximation and is limited by vertebral asymmetry.
Magnetic Resonance Imaging
-
Imaging should extend from the posterior fossa to the conus medullaris.
-
Purpose is to exclude intraspinal pathology.
-
Indications include:
-
Atypical curve patterns
-
Rapid progression
-
Excessive kyphosis
-
Neurological symptoms
-
Foot deformities
-
Asymmetric abdominal reflexes
-
Classification Systems
-
Schulthess classification
-
Ponseti and Friedman classification
-
King–Moe classification
-
Lenke classification (most widely used)
Lenke Classification
-
Based on:
-
Identification of the primary curve
-
Lumbar modifier
-
Thoracic sagittal modifier
-
-
Helps determine which curves require inclusion in the fusion construct.
-
Allows standardized surgical planning.
Management Considerations
-
Remaining growth potential
-
Curve magnitude and pattern
-
Risk of progression
-
Sex and genetic risk profile
Non-Surgical Management
Observation
-
Indicated for curves less than 25 degrees.
-
Regular clinical and radiographic follow-up is essential.
-
Frequency depends on curve magnitude and skeletal maturity.
Bracing
-
Indicated for progressive curves between 25 and 40 degrees in skeletally immature patients.
-
Goal is to prevent progression, not to correct the curve.
-
Commonly used braces include:
-
Cervicothoracolumbosacral orthosis
-
Thoracolumbosacral orthosis
-
Night-time bending braces
-
-
Compliance is critical for success.
Surgical Management
Indications
-
Progressive curves greater than 40 degrees in skeletally immature patients
-
Curves greater than 50 degrees at skeletal maturity
Surgical Options
-
Posterior spinal instrumentation and fusion
-
Anterior spinal fusion
-
Combined anterior and posterior fusion in selected cases
Goals of Surgery
-
Correction of deformity
-
Maintenance of coronal and sagittal balance
-
Preservation of pulmonary function
-
Minimization of pain and complications
-
Preservation of lumbar spine function
Complications
-
Neurological injury
-
Blood loss
-
Pseudarthrosis
-
Implant-related complications
-
Infection
-
Flat back syndrome
-
Superior mesenteric artery syndrome
-
Crankshaft phenomenon in skeletally immature patients
Courtesy: Harry Benjamin Laing, MRCS, UK
Leave a Reply