Courtesy: Prof Young Lae Moon, Seoul, South Korea
Comprehensive Shoulder Physical Examination
Orthopaedic Principles – Webinar Summary
1. Introduction
-
A systematic shoulder examination is essential for accurate diagnosis and treatment planning.
-
A structured, stepwise approach improves diagnostic precision and reduces missed pathology.
-
Key focus:
-
Cervical spine assessment
-
Rotator cuff evaluation
-
Shoulder instability assessment
-
2. Core Principles of Shoulder Examination
2.1 Rule Out Cervical Spine Pathology
-
Essential to differentiate:
-
Referred pain from cervical spine
-
True shoulder pathology
-
-
Components:
-
Cervical range of motion
-
Neurological examination
-
Provocative testing
-
Spurling Test
-
Purpose: Detect cervical radiculopathy
-
Technique:
-
Neck extension + lateral bending + rotation toward symptomatic side
-
Apply axial compression (~7 kg)
-
-
Positive Test:
-
Radicular pain radiating into the arm (not just neck pain)
-
-
Evidence:
-
High specificity (~90–95%) for cervical radiculopathy (supported by current literature)
-
Neurological Correlation
-
C5: Deltoid (shoulder abduction)
-
C6: Biceps, wrist extension
-
C7: Triceps, wrist extension
3. Range of Motion & Capsular Patterns
Adhesive Capsulitis (Frozen Shoulder)
-
Characteristic pattern:
-
Marked restriction in abduction
-
Relative preservation of forward flexion
-
-
Clinical relevance:
-
Helps differentiate from rotator cuff pathology
-
-
Evidence update:
-
Classical capsular pattern (ER > abduction > IR restriction) remains widely accepted
-
4. Subacromial Impingement
4.1 Neer Impingement Test
-
Technique:
-
Passive forward elevation with internal rotation
-
Stabilize scapula
-
-
Positive Test:
-
Pain between 70°–130° elevation
-
-
Indicates:
-
Subacromial impingement
-
4.2 Types of Impingement
Primary Impingement
-
Cause:
-
Structural narrowing (acromion, osteophytes)
-
-
Mechanism:
-
Compression of rotator cuff and subacromial bursa
-
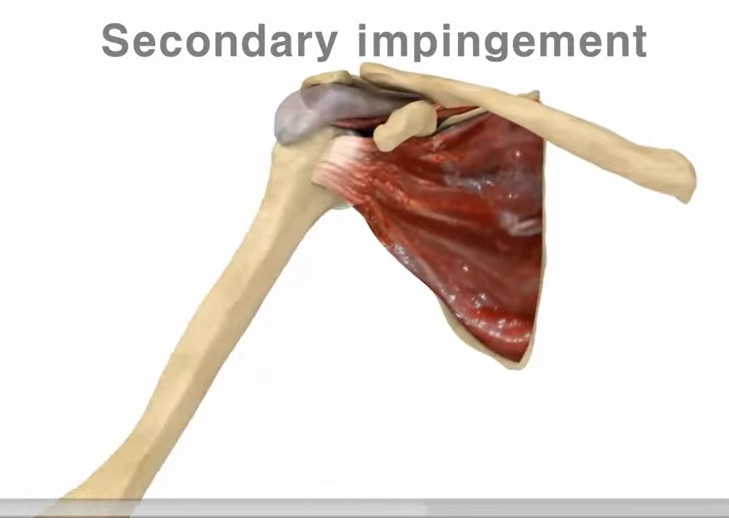
Secondary Impingement
-
Cause:
-
Rotator cuff weakness
-
-
Mechanism:
-
Superior migration of humeral head
-
Functional instability
-
-
Clinical importance:
-
Requires different treatment approach than primary impingement
-
5. Rotator Cuff Evaluation
5.1 Supraspinatus
Empty Can (Jobe) Test
-
Arm at 90° abduction in scapular plane, thumb down
-
Positive:
-
Pain or weakness
-
-
Evidence:
-
High sensitivity for supraspinatus pathology
-
Drop Arm Test
-
Passive abduction ? slow controlled lowering
-
Positive:
-
Sudden drop or inability to control descent
-
-
Indicates:
-
Full-thickness tear
-
-
High specificity (~95%)
5.2 Subscapularis
Belly Press Test
-
Press abdomen while keeping elbow forward
-
Positive:
-
Elbow drops backward / wrist flexion compensation
-
-
High specificity (~90–98%)
Lift-Off Test
-
Hand behind back ? lift away
-
Positive:
-
Inability or weakness
-
-
Best for:
-
Lower subscapularis tears
-
Clinical Note (Updated Evidence):
-
Bear Hug Test (not demonstrated but discussed):
-
More sensitive for upper subscapularis tears
-
-
Combining tests improves diagnostic accuracy (supported by recent literature)
5.3 Infraspinatus & Teres Minor
External Rotation Strength Test
-
Resisted external rotation
-
Positive:
-
Weakness or pain
-
External Rotation Lag Sign
-
Inability to maintain external rotation
-
Suggests:
-
Significant posterior cuff tear
-
Hornblower’s Sign
-
Arm at 90° abduction ? external rotation
-
Positive:
-
Inability to externally rotate
-
-
Indicates:
-
Teres minor involvement / massive cuff tear
-
-
High specificity (~95%)
6. Shoulder Instability
6.1 Anterior Instability
Apprehension Test
-
Arm in 90° abduction + external rotation
-
Positive:
-
Apprehension (fear of dislocation, not just pain)
-
Relocation Test
-
Posterior pressure relieves symptoms
-
Confirms:
-
Anterior instability
-
6.2 Translation Tests
Anterior & Posterior Drawer Tests
-
Assess humeral head translation
-
Helps quantify instability
6.3 Posterior Instability
-
Posteriorly directed force
-
Positive:
-
Excessive posterior translation or symptoms
-
6.4 Multidirectional Instability (MDI)
Sulcus Sign
-
Downward traction on arm
-
Positive:
-
Visible sulcus below acromion
-
-
Indicates:
-
Inferior capsular laxity
-
7. Biceps Tendon Evaluation
7.1 Speed’s Test
-
Forward flexion + supination against resistance
-
Positive:
-
Pain in bicipital groove
-
-
Indicates:
-
Long head of biceps tendinopathy
-
7.2 Yergason’s Test
-
Resisted supination + external rotation
-
Positive:
-
Pain or snapping
-
-
Indicates:
-
Biceps instability or subluxation
-
Clinical Insight
-
Biceps pathology is often associated with:
-
Subscapularis tears
-
Pulley lesions
-
8. Diagnostic Injections
-
Purpose: Identify pain generator
-
Common targets:
-
Glenohumeral joint
-
Subacromial space
-
Biceps tendon sheath
-
Suprascapular nerve
-
-
Interpretation:
-
Pain relief ? confirms source of pathology
-
-
Evidence:
-
Widely supported as a diagnostic adjunct in shoulder practice
-
9. Key Takeaways
-
Always follow a systematic approach:
-
Rule out cervical pathology
-
Assess rotator cuff
-
Evaluate instability
-
-
Understand functional anatomy to interpret tests correctly
-
Use clusters of tests rather than relying on a single test
-
Consider diagnostic injections when diagnosis is unclear
10. Expert Clinical Insight
-
Belly press test preferred for subscapularis assessment in routine practice
-
Imaging (MRI/Ultrasound) should be used when:
-
Clinical findings are equivocal
-
Partial tears are suspected
-

Leave a Reply