Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Ulnar Claw Hand
Definition
Ulnar claw hand is an abnormal hand posture caused by injury to the ulnar nerve, most commonly from a distal (low) ulnar nerve lesion.
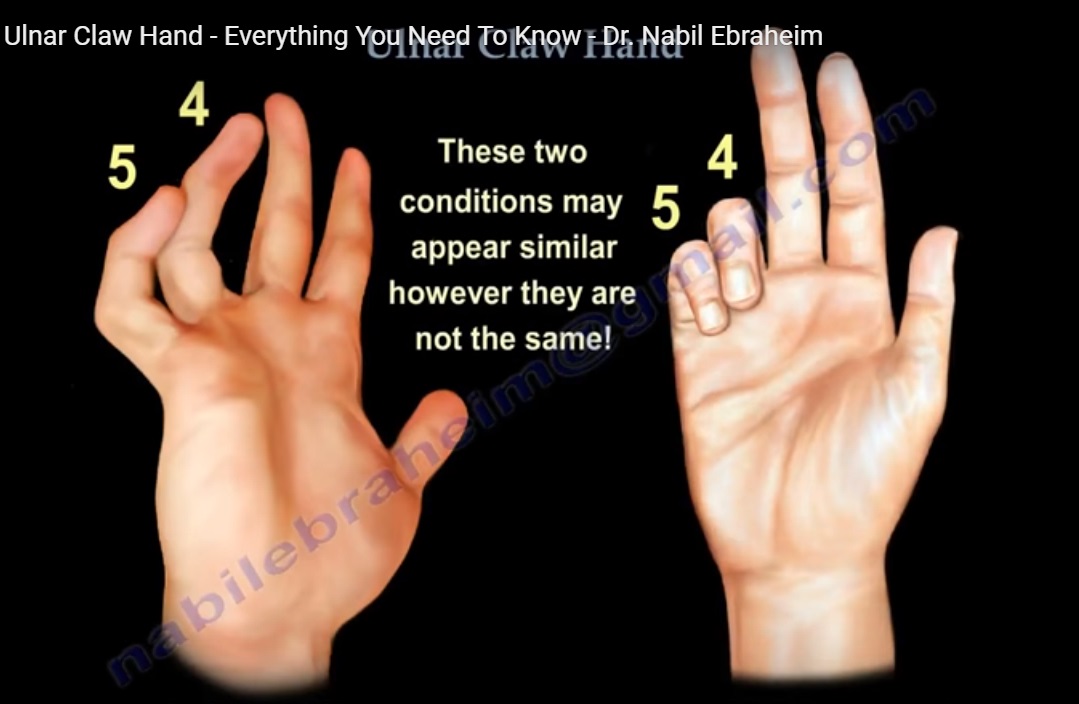
It is characterized by clawing of the:
- Ring finger (4th digit)
- Little finger (5th digit)
Clinical Features
The deformity becomes most obvious when the patient attempts finger extension.
Typical posture includes:
- Hyperextension at the MCP joints
- Flexion at the PIP and DIP joints
The deformity predominantly affects:
- Ring finger
- Little finger
Pathophysiology
The deformity results from paralysis of:
- Interossei muscles
- Ulnar two lumbricals (4th and 5th digits)
Normal Function of These Muscles
The intrinsic muscles normally:
- Flex the MCP joints
- Extend the IP joints
Mechanism of Clawing
Loss of intrinsic muscle function produces imbalance between intrinsic and extrinsic muscles.
This results in:
- Unopposed Extensor Digitorum Communis (EDC)
- Causes MCP hyperextension
- Unopposed Flexor Digitorum Profundus (FDP)
- Causes flexion at PIP and DIP joints
The final posture is the classic claw deformity.
Low vs High Ulnar Nerve Lesion
Low Ulnar Nerve Lesion
Location
- Wrist-level lesion
Findings
The FDP to the ring and little fingers remains intact.
Features include:
- More prominent clawing
- Preserved sensation over dorsum of hand
This occurs because the dorsal cutaneous branch is spared.
Clinical Memory Aid
“Low lesion = more clawing”
High Ulnar Nerve Lesion
Location
- Above elbow
Findings
The FDP to the ring and little fingers is also paralyzed.
Features include:
- Less clawing deformity
- Loss of sensation over dorsum of hand
Ulnar Paradox
Despite being a more severe lesion, the clawing appears less obvious because the FDP is weak.
This is called the:
- Ulnar paradox
Clinical Memory Aid
“High lesion = less clawing”
Why the Index and Middle Fingers are Spared
The lumbricals to the:
- Index finger
- Middle finger
are supplied by the median nerve.
These lumbricals maintain:
- MCP flexion
- IP extension
Therefore, clawing is prevented in these digits.
Comparison with Intrinsic Minus Hand
Ulnar Claw Hand
Features
- Only ring and little fingers affected
- Due to ulnar nerve injury
Intrinsic Minus Hand (True Claw Hand)
Features
- All fingers affected
- Represents generalized intrinsic muscle loss
Causes
Common causes include:
- Volkmann ischemic contracture
- Compartment syndrome
- Charcot-Marie-Tooth disease
- Leprosy
- Improper splinting after trauma
Key Biomechanical Concept
The claw deformity occurs because of:
- Weak intrinsic muscles
- Strong extrinsic muscles
Muscle Imbalance
Extensor Digitorum Communis (EDC)
- Produces MCP hyperextension
FDP and FDS
- Produce flexion of PIP and DIP joints
Final Hand Posture
The characteristic deformity consists of:
- MCP hyperextension
- PIP and DIP flexion
primarily involving the ring and little fingers.


Leave a Reply