Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Clavicle Fracture Classification: Allman & Neer Systems
Introduction
Clavicle fractures are common injuries, traditionally treated conservatively.
However, current evidence suggests that displaced fractures may benefit from surgical fixation.
Why This Matters
Conservative treatment of significantly displaced fractures may lead to:
- Malunion
- Nonunion
- Persistent shoulder dysfunction
Anatomy Relevant to Stability
Coracoclavicular (CC) Ligaments
The primary stabilizers of the distal clavicle, preventing superior displacement.
Components
- Conoid ligament — medial
- Trapezoid ligament — lateral
Clinical Importance
Integrity of CC ligaments determines:
- Stability
- Need for surgery
Allman Classification
Overview
Classifies clavicle fractures based on anatomical location into three groups:
Group I – Middle Third Fractures
Epidemiology
- ~80% of all clavicle fractures
- Most common type
Mechanism of Displacement
Medial Fragment
- Pulled superiorly by sternocleidomastoid
Lateral Fragment
- Displaced inferiorly due to:
- Weight of arm
- Gravity
- Shoulder muscle pull
Management
Nonoperative Treatment
- Sling immobilization
- Suitable for minimally displaced fractures
Indications for Surgery
- Displacement >100%
- Shortening >2 cm
- Open fracture
- Neurovascular injury
- Symptomatic nonunion
Group II – Lateral Third Fractures
Epidemiology
- 10–15% of clavicle fractures
Key Concept
Stability depends on CC ligament integrity
Neer Classification of Distal Clavicle Fractures
Type I
Features
- Fracture lateral to CC ligaments
- Ligaments intact
- Minimal displacement
Stability
- Stable
Treatment
- Conservative
Type IIA
Features
- Fracture medial to CC ligaments
- Ligaments attached to distal fragment
Stability
- Medial fragment unstable
Risk
- High risk of nonunion
Treatment
- Often surgical
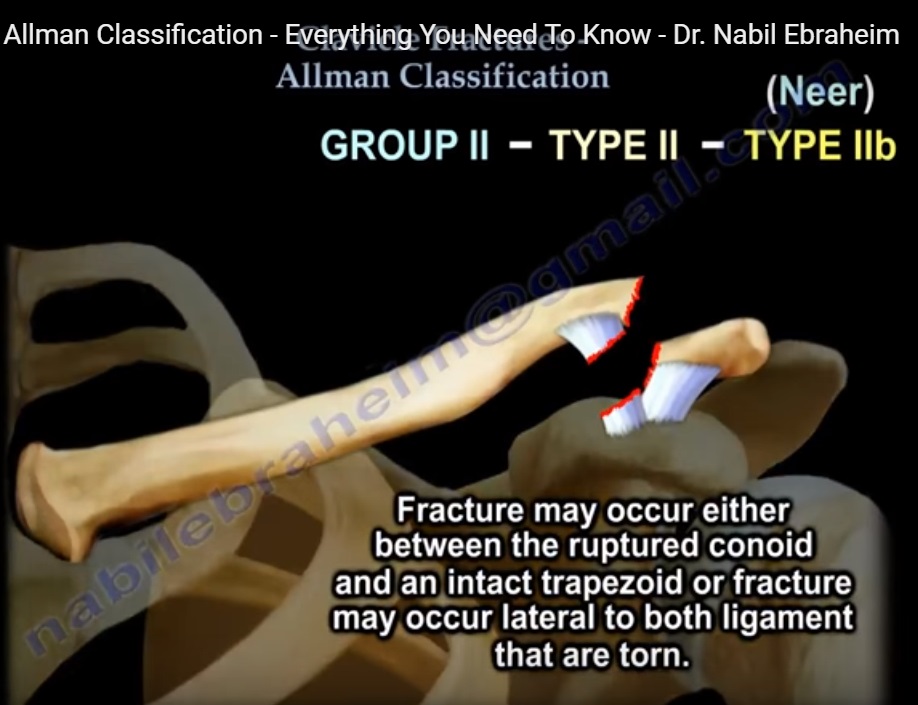
Type IIB
Features
- Fracture between conoid and trapezoid
OR - Lateral fracture with ligament rupture
Stability
- Conoid ligament disrupted
- Medial fragment unstable
Risk
- Very high nonunion rate
Treatment
- Surgical fixation required
Type III
Features
- Intra-articular (AC joint involvement)
- Ligaments intact
Stability
- Stable
Complication
- Post-traumatic AC arthritis
Treatment
- Conservative
Group III – Medial Third Fractures
Epidemiology
- ~5% of clavicle fractures
Characteristics
- Usually minimally displaced
- Rarely progress to nonunion
Management
- Sling immobilization
- Nonoperative in most cases
Summary Table
| Allman Group | Location | Frequency | Stability | Treatment |
|---|---|---|---|---|
| Group I | Middle third | ~80% | Variable | Conservative or surgery if displaced |
| Group II | Lateral third | 10–15% | Depends on CC ligaments | Guided by Neer classification |
| Group III | Medial third | ~5% | Usually stable | Conservative |
Key Clinical Points
High-Yield Concepts
- Midshaft fractures- most common
- Distal fractures with CC ligament injury – high nonunion risk
- Neer Type II fractures – usually require surgery
- Medial fractures – rare and typically stable
Clinical Insight
Always assess:
- Degree of displacement
- Ligament integrity
These determine:
- Stability
- Treatment strategy


Leave a Reply