‘
Courtesy: Michell Ruiz, Mexico
Chronic Shoulder Dislocations
Current Concepts in Diagnosis and Management
Chronic shoulder dislocations remain one of the most challenging conditions in shoulder surgery. Delayed diagnosis, complex pathology, and variable presentation require an individualized treatment strategy based on patient factors, chronicity, and associated injuries.
Epidemiology
Acute Shoulder Dislocations
- Anterior dislocations: Approximately 95%
- Posterior dislocations: Approximately 5%
Chronic Shoulder Dislocations
- Often underdiagnosed, particularly posterior dislocations
- More frequently encountered in developing countries due to:
- Delayed presentation
- Limited access to healthcare
- Missed initial diagnosis
- True prevalence is likely underestimated.
Definition of Chronic Shoulder Dislocation
A chronic shoulder dislocation is generally considered one that:
- Is missed during the initial evaluation
- Presents with delayed treatment
- Usually cannot be reduced by closed methods
- Frequently requires open surgical management after approximately 3 weeks from injury.
Clinical Evaluation
Patient Assessment
Treatment should be individualized based on:
- Duration of dislocation
- Patient age
- Functional demands
- Comorbidities
- Psychological status
- Degree of disability
Imaging Evaluation
Initial Imaging
Standard radiographs include:
- True AP view
- Axillary view
- Scapular Y view
Advanced Imaging
CT Scan with CT Angiography
Used to evaluate:
- Glenoid bone loss
- Humeral head defects
- Axillary artery location
- Posterior circumflex humeral artery patency
MRI
Useful for assessing:
- Rotator cuff integrity
- Fatty degeneration
- Humeral head vascularity
- Associated soft tissue injuries
CT angiography and MRI together provide the information required for surgical planning.
Principles of Management
Non-operative Treatment
May be considered in selected chronic anterior dislocations with:
- Minimal symptoms
- Low functional demands
- Mild improvement after physiotherapy
Posterior locked dislocations rarely benefit from conservative treatment.
Surgical Management
Treatment depends on:
- Chronicity
- Bone loss
- Rotator cuff status
- Vascularity of the humeral head
- Associated lesions
Surgical options include:
- Open reduction
- Capsulolabral repair
- Remplissage
- Bone grafting
- Tendon transfer
- Reverse shoulder arthroplasty
- Anatomical arthroplasty (selected cases)
Management of Chronic Anterior Shoulder Dislocations
Surgical Principles
- Complete release of capsular fibrosis
- Circumferential glenoid release
- Careful protection of the axillary neurovascular structures
- Preservation of the native humeral head whenever feasible
- Repair of the subscapularis tendon
- Rotator interval closure
- Remplissage for engaging Hill-Sachs lesions
- Iliac crest bone grafting for significant anterior glenoid defects
Procedures to Avoid
- Routine Latarjet procedure
- Coracoid osteotomy
- Transarticular fixation wires
These techniques may increase complications without improving outcomes in chronic dislocations.
Reverse Shoulder Arthroplasty
Indications
Reverse arthroplasty is considered when:
- Humeral head defect exceeds 25%
- Poor humeral head vascularity
- Advanced avascular necrosis
- Severe rotator cuff insufficiency
Preservation of native anatomy remains the preferred option whenever possible.
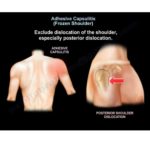
Management of Chronic Posterior Shoulder Dislocations
Common Pathological Features
- Reverse Hill-Sachs (McLaughlin) lesion
- Posterior capsular laxity
- Glenoid bone loss
- Pectoralis major contracture
- Axillary nerve compression
- Posterior instability
Surgical Strategy
- Deltopectoral approach in most cases
- Posterior capsulolabral repair when required
- Reverse remplissage
- Structural bone grafting for large humeral defects
Routine modified McLaughlin procedures are not preferred in the author’s current practice.
Key Surgical Pearls
Successful surgery depends on:
- Accurate preoperative imaging
- Thorough capsular release
- Stable humeral head reduction
- Appropriate management of bone loss
- Rotator cuff preservation
- Restoration of shoulder stability
- Individualized treatment planning
Key Takeaways
- Chronic shoulder dislocations remain a significant reconstructive challenge.
- Delayed diagnosis is the leading cause of poor outcomes.
- CT angiography has become an important tool for surgical decision-making.
- Native humeral head preservation should be attempted whenever feasible.
- Reverse shoulder arthroplasty should be reserved for selected patients with severe bone loss or compromised vascularity.
- Treatment should always be individualized according to patient characteristics and associated pathology.
.

Leave a Reply