Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
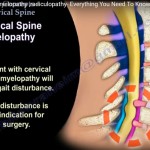
Cervical Myelopathy vs Cervical Radiculopathy
Introduction
Cervical spine pathology may produce either:
- Cervical myelopathy (spinal cord compression)
- Cervical radiculopathy (nerve root compression)
Differentiating the two is critical because cervical myelopathy is a neurological emergency that may require urgent surgical treatment.
Part 1: Cervical Myelopathy
Definition
Cervical myelopathy results from compression of the cervical spinal cord.
It commonly occurs due to:
- Cervical spondylosis
- Disc degeneration
- Ossification of ligaments
- Multilevel canal stenosis
Key Clinical Features
Most Important Red Flag
Gait disturbance should be considered cervical myelopathy until proven otherwise.
Symptoms
Common symptoms include:
- Gait instability
- Spastic gait
- Hand clumsiness
- Loss of fine motor control
- Upper limb weakness
- Neck pain
- Neck stiffness
Upper Motor Neuron Signs
Typical examination findings include:
- Hyperreflexia
- Spasticity
- Clonus
- Positive Babinski sign
- Positive Hoffmann sign
These indicate spinal cord involvement.
Hoffmann Sign
The Hoffmann sign is a finger flexion reflex suggestive of cervical cord compression.
It is elicited by flicking the distal phalanx of the middle finger.
A positive test produces:
- Flexion of thumb and index finger
Investigations
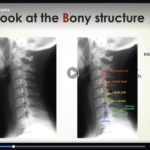
X-ray Findings
May demonstrate:
- Cervical spondylosis
- Loss of cervical lordosis
- Cervical kyphosis
- Degenerative changes
MRI
MRI is the gold standard investigation.
It demonstrates:
- Cord compression
- Disc pathology
- Canal stenosis
- Cord signal changes
Cord signal change is generally a late finding and may indicate worse prognosis.
Important Clinical Pitfall
A patient with:
- Low back pain
- Lumbar stenosis on MRI
- Gait disturbance
should always undergo cervical spine evaluation to exclude tandem stenosis.
Surgical Indications
Indications for surgery include:
- Gait disturbance
- Progressive neurological deficit
- Significant cord compression
- Functional deterioration
Surgical Approaches
Anterior Approach
Preferred when there is:
- Kyphosis greater than 10°
- One- or two-level disease
- Need for deformity correction
Posterior Approach
Includes:
- Laminectomy with or without fusion
Typically used for:
- Multilevel compression
Important Limitation
Posterior decompression is generally contraindicated in fixed kyphosis greater than 10°.
Laminectomy alone may lead to:
- Postoperative kyphosis
Laminoplasty
Used for:
- Multilevel cervical stenosis
Not suitable for:
- Fixed cervical kyphosis
Complications
C5 Palsy
One of the most common complications.
Features include:
- Deltoid weakness
- Shoulder abduction weakness
Recovery is often delayed.
Infection
More common after posterior surgery.
Airway Compromise
Risk increases with:
- Surgery longer than 5 hours
- More than 3 operative levels
- Blood loss greater than 300 ml
Intraoperative Monitoring
Somatosensory Evoked Potentials (SSEP)
Significant warning signs include:
- Greater than 50% reduction in amplitude
- Greater than 10% increase in latency
Nerve Injuries During Cervical Surgery
Recurrent Laryngeal Nerve Injury
May cause:
- Hoarseness
- Vocal cord paralysis
Superior Laryngeal Nerve Injury
May produce:
- Loss of high-pitched voice
Particularly important in singers and professional voice users.
Cervical Spine Biomechanics
Rotation
Approximately 50% of cervical rotation occurs at:
- C1–C2
Flexion and Extension
Maximum motion occurs at:
- C4–C5
Part 2: Cervical Radiculopathy
Definition
Cervical radiculopathy occurs due to compression or irritation of a cervical nerve root.
Clinical Features
Symptoms typically include:
- Neck pain radiating into one arm
- Dermatomal numbness
- Paresthesia
- Weakness
Important Clinical Sign
Shoulder Abduction Relief Test
The patient places the hand over the head.
Relief of symptoms suggests:
- Cervical nerve root irritation
This is also called the shoulder abduction sign.
Important Anatomical Concept
Cervical nerve roots are relatively horizontal.
A cervical disc herniation usually affects the nerve root at the same level.
Example:
- C6–C7 disc herniation affects the C7 nerve root
Dermatomes, Myotomes, and Reflexes
C5 Root
Motor
- Shoulder abduction (deltoid)
Reflex
- Biceps reflex
C6 Root
Sensory
- Thumb
- Index finger
Motor
- Wrist extension
Reflex
- Brachioradialis reflex
C7 Root
Sensory
- Middle finger
Motor
- Elbow extension (triceps)
- Wrist flexion
- Finger extension
Reflex
- Triceps reflex
C8 Root
Sensory
- Little finger
Motor
- Finger flexion
- Grip strength
Reflex
- No reliable reflex
T1 Root
Motor
- Interossei muscles
- Finger abduction and adduction
Examination Tests
Spurling Test
Neck extension with axial compression reproduces radicular symptoms.
A positive test suggests cervical radiculopathy.
Shoulder Abduction Test
Relief of symptoms supports cervical nerve root pathology.
Management
Conservative Treatment
Initial management includes:
- NSAIDs
- Physiotherapy
- Activity modification
Approximately 75% improve without surgery.
Surgical Indications
Surgery is considered for:
- Persistent pain beyond 6–12 weeks
- Progressive neurological deficit
- Significant weakness
Key Clinical Pearls
- Gait disturbance suggests cervical myelopathy until proven otherwise.
- Cervical myelopathy produces upper motor neuron signs.
- C6–C7 disc herniation commonly causes C7 radiculopathy.
- Middle finger numbness suggests C7 involvement.
- Thumb and index finger symptoms suggest C6 involvement.
- False-positive MRI findings are common; always correlate clinically.
- There are 7 cervical vertebrae but 8 cervical nerve roots.


Leave a Reply