Courtesy: Anny Hsu, MD, Assistant Professor, New York Medical College, New York, USA
Overview of Cavovarus Foot Deformity
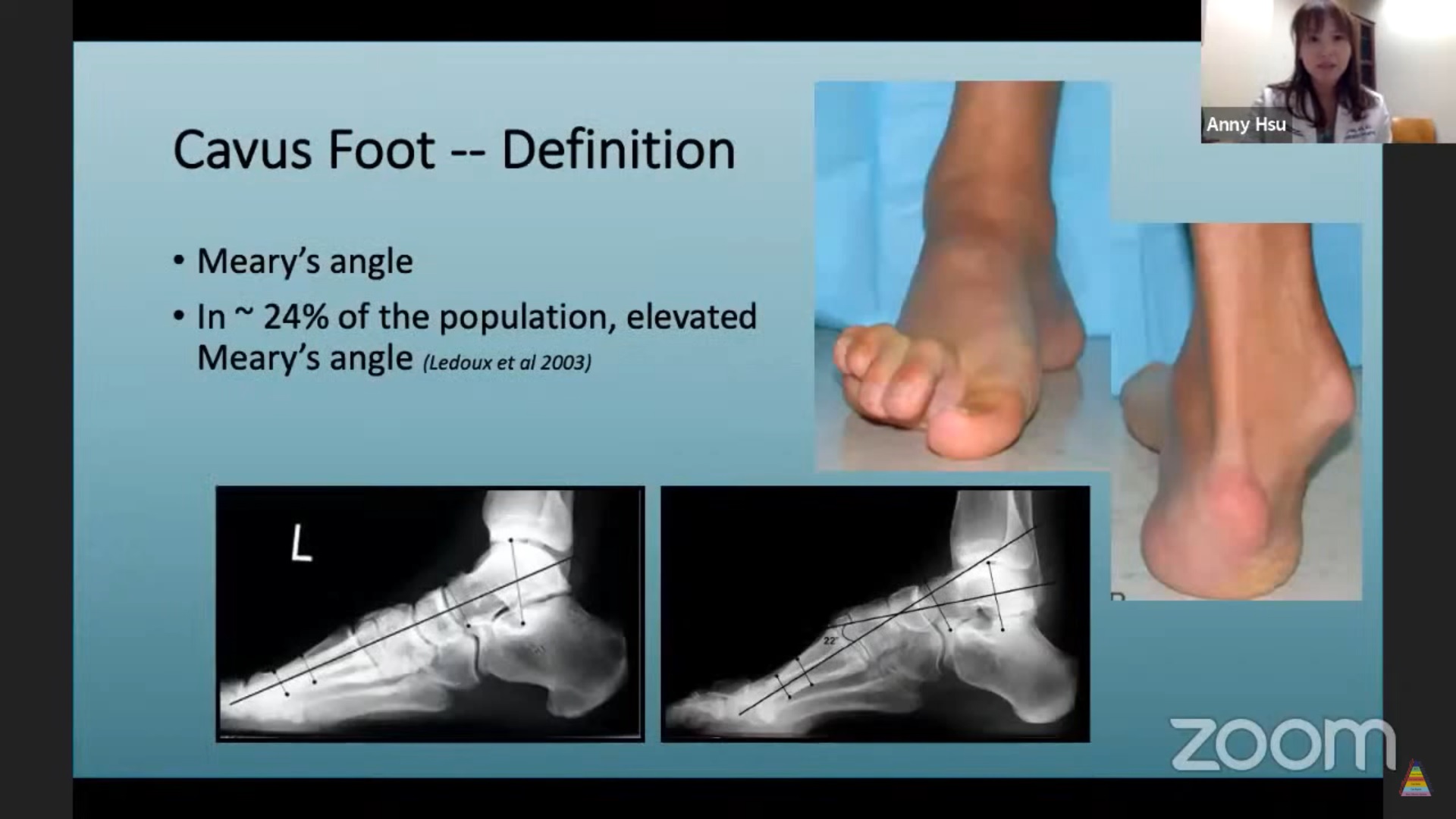
Cavovarus deformity is defined by:
-
Increased Meary’s angle
-
Dorsal apex angulation
-
Plantarflexed first ray
-
Varus hindfoot alignment
Although an elevated Meary’s angle can be seen in up to 24% of the population, clinically significant cavovarus deformity results in pain, instability, and progressive secondary pathology.
Etiology
Neurogenic Causes (Most Common)
-
Charcot–Marie–Tooth disease
-
Stroke
-
Poliomyelitis
-
Cerebral palsy
-
Friedreich’s ataxia
-
Spinal cord lesions
-
Spinal muscular atrophy
Congenital Causes
-
Residual or relapsed clubfoot
-
Arthrogryposis
Acquired / Post-Traumatic Causes
-
Burns
-
Compartment syndrome
-
Crush injuries
-
Talar fracture malunion
-
Peroneal nerve injury
-
Peroneal tendon insufficiency
Clinical Presentation
Patients often adapt to the deformity and present with secondary complaints, including:
-
Lateral ankle instability (“ankle giving way”)
-
Peroneal tendinopathy
-
Sesamoiditis
-
Metatarsalgia
-
Fifth metatarsal stress fractures
-
Plantar calluses and ulceration
-
Progressive medial compartment knee arthritis (long-term)
Biomechanics of Cavovarus Foot
-
Hyperactive peroneus longus plantarflexes the first ray
-
Loss of normal tripod weight bearing
-
Subtalar joint is pulled into varus, becoming rigid over time
-
Hindfoot varus becomes fixed and progressive
Clinical Examination
Key Findings
-
Peek-a-boo heel sign (visible heel varus from the front)
-
Apparent neutral heel may mask subtalar eversion compensation
-
Weak eversion strength
-
Clawing of toes in severe or neurogenic cases
Coleman Block Test
A critical test to differentiate:
-
Forefoot-driven flexible hindfoot varus
-
True fixed hindfoot varus
This test directly influences surgical decision-making.
Radiographic Evaluation
Hindfoot
-
Increased calcaneal pitch (lateral view)
-
Decreased talar–calcaneal angle (AP view)
-
Harris axial view to quantify hindfoot varus
Midfoot
-
Elevated navicular height
-
Increased medial–lateral forefoot imbalance
-
Talonavicular joint subluxation is common
Non-Operative Management
Initial management includes:
-
Gastrocnemius stretching
-
Custom orthotics:
-
Lateral hindfoot posting
-
Low medial arch
-
First-ray recess to accommodate plantarflexion
-
Flexible deformities may respond well; rigid deformities usually do not.
Principles of Surgical Planning
Cavovarus correction is three-dimensional and complex. Key considerations include:
-
Flexibility of deformity (Coleman block test)
-
Presence of arthritis (CT scan if needed)
-
Equinus contracture (present in ~99%)
-
Neurologic etiology (risk of recurrence)
-
Associated ankle instability
-
Ankle alignment (standing ankle X-ray mandatory)
?? Failure to identify a neurologic cause may result in recurrence.
Soft Tissue Procedures
Equinus Correction
-
Gastrocnemius recession
-
Percutaneous or open Achilles tendon lengthening
-
Posterior capsular release (for severe stiffness)
Tendon Balancing
-
Peroneus longus ? brevis transfer
-
Posterior tibial tendon lengthening or transfer
-
Jones procedure for clawed hallux
-
Flexor tenotomies for severe claw toes
Bony Procedures
Hindfoot
-
Lateralizing calcaneal osteotomy (preferred)
-
Dwyer closing wedge osteotomy (less favored in adults)
Forefoot
-
First metatarsal dorsiflexion osteotomy
-
Maintain plantar hinge
-
Avoid shortening or rotational malalignment
-
Severe Deformities
-
Lateral column shortening (selectively)
-
Midfoot dorsal wedge osteotomy (Japas-type)
-
Talar neck osteotomy for talar malunion
-
Supramalleolar osteotomy for ankle varus
Arthrodesis
Indicated for rigid deformity with arthritis:
-
Subtalar fusion
-
Triple arthrodesis
Operative Setup & Technical Pearls
-
Supine positioning, thigh tourniquet
-
Fluoroscopy essential
-
Address Achilles pathology first
-
Perform bony correction before tendon balancing
-
Intraoperative simulated weight bearing helps avoid undercorrection
Post-Operative Rehabilitation
-
2–3 weeks: splint
-
3 weeks: cast
-
6 weeks: boot, partial weight bearing
-
10–12 weeks: full weight bearing
-
Gradual return to sport after additional therapy
Case Discussions
Case 1: Post-Traumatic Cavovarus with Plantar Ulcer
-
Percutaneous Achilles lengthening
-
MIS calcaneal osteotomy
-
First metatarsal dorsiflexion osteotomy
-
Peroneus longus ? brevis transfer
-
Lateral ligament repair
Outcome: Pain relief, ulcer resolution, restored function.
Case 2: Rigid Cavovarus with Post-Traumatic Arthritis
-
Endoscopic gastrocnemius recession
-
Hardware removal
-
Triple arthrodesis
-
First metatarsal dorsiflexion osteotomy
Outcome: Stable alignment, pain resolution.
Key Take-Home Messages
-
Cavovarus deformity requires systematic evaluation
-
Always rule out neurologic causes
-
Coleman block test is critical
-
Address equinus and bony alignment first
-
Tendon balancing fine-tunes correction
-
Under-correction is more common than over-correction


Leave a Reply