Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Basic Structure of the Brachial Plexus
- Brachial plexus formed from nerve roots C5–T1.
- Organization follows: Roots ? Trunks ? Divisions ? Cords ? Branches.
- Five roots: C5, C6, C7, C8, T1.
Trunks
- C5 + C6 join to form the Upper trunk.
- C7 continues alone as the Middle trunk.
- C8 + T1 join to form the Lower trunk.
Divisions
- Each trunk divides into an anterior and posterior division.
- Posterior divisions of all three trunks unite to form the Posterior cord.
- Anterior divisions of upper and middle trunks form the Lateral cord.
- Anterior division of the lower trunk forms the Medial cord.
Cords
- Named according to relation to the axillary artery.
- Lateral cord – lateral to axillary artery.
- Posterior cord – posterior to axillary artery.
- Medial cord – medial to axillary artery.
Branches from Roots (Preclavicular Branches)
- Dorsal scapular nerve (C5) – supplies rhomboids and levator scapulae.
- Long thoracic nerve (C5–C7) – supplies serratus anterior.
- Injury causes medial winging of the scapula.
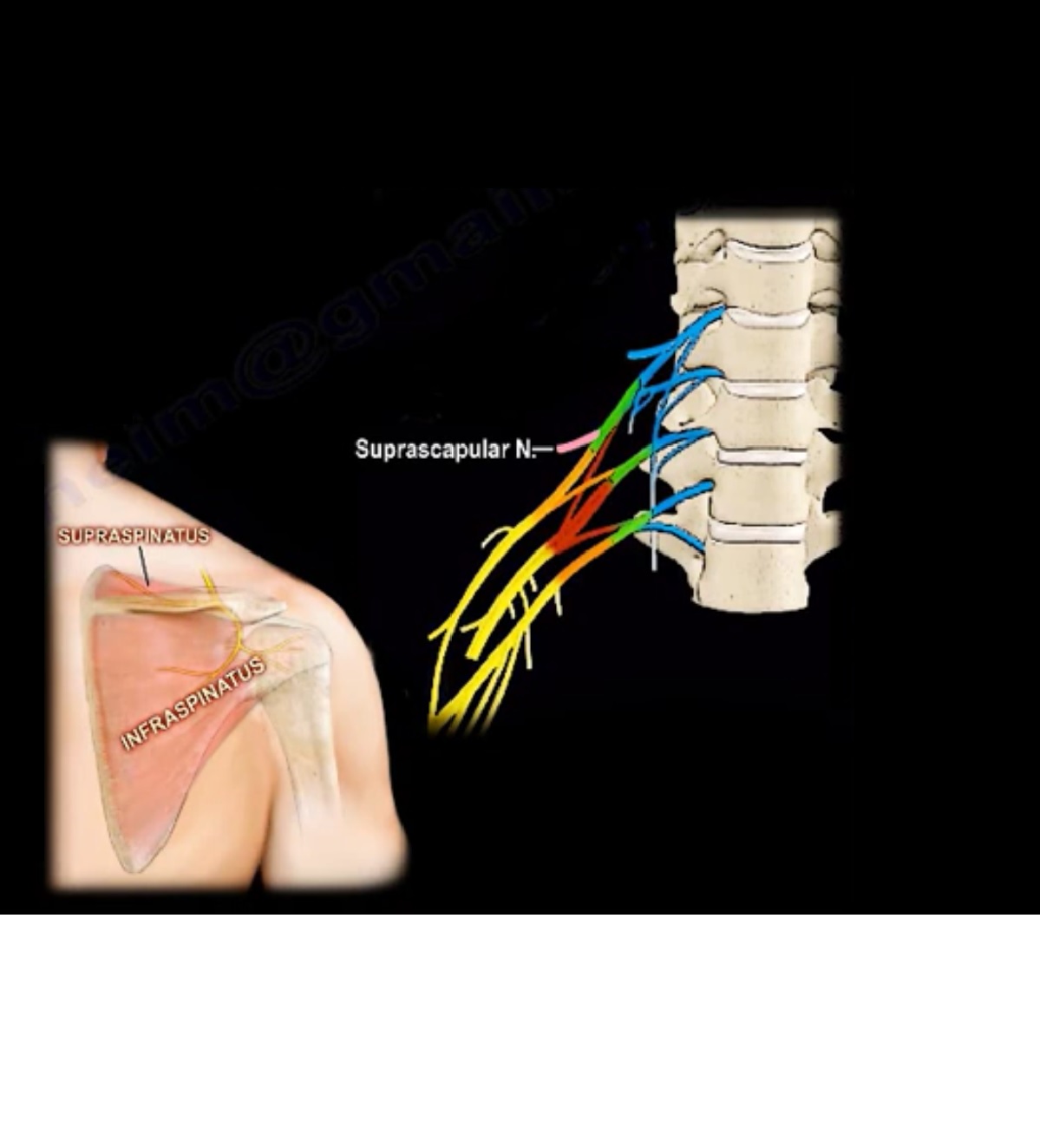
Branches from Upper Trunk
- Suprascapular nerve – supplies supraspinatus and infraspinatus.
- Nerve to subclavius.
Branches from Lateral Cord
- Lateral pectoral nerve.
- Musculocutaneous nerve.
- Lateral root of the median nerve.
Branches from Posterior Cord
- Upper subscapular nerve – supplies subscapularis.
- Thoracodorsal nerve – supplies latissimus dorsi.
- Lower subscapular nerve – supplies subscapularis and teres major.
- Axillary nerve – supplies deltoid and teres minor.
- Radial nerve – supplies posterior arm and forearm muscles.
Branches from Medial Cord
- Medial pectoral nerve.
- Medial cutaneous nerve of arm.
- Medial cutaneous nerve of forearm.
- Ulnar nerve.
- Medial root of the median nerve.
Median Nerve Formation
- Formed by union of lateral root (from lateral cord) and medial root (from medial cord).
Preganglionic vs Postganglionic Brachial Plexus Injury
- Preganglionic injury occurs proximal to dorsal root ganglion (root avulsion).
- Involves central nervous system.
- Has poor prognosis and no potential for recovery.
- Postganglionic injury occurs distal to dorsal root ganglion.
- Involves peripheral nervous system.
- Has potential for regeneration and better prognosis.
Signs of Preganglionic Injury
- Horner syndrome (ptosis, miosis, anhidrosis, enophthalmos).
- Medial scapular winging due to long thoracic nerve involvement.
- Rhomboid paralysis due to dorsal scapular nerve injury.
- Supraspinatus and infraspinatus weakness.
- Sensation preserved because dorsal root ganglion intact.
Signs of Postganglionic Injury
- Both motor and sensory deficits present.
- Injury usually post?clavicular.
- EMG shows intact cervical paraspinal innervation.
Erb’s Palsy
- Injury to upper trunk (C5–C6).
- Causes weakness of deltoid, rotator cuff, elbow flexors, and wrist extensors.
- Arm position: adducted, internally rotated shoulder, extended elbow, pronated forearm.
- Classic appearance called ‘Waiter’s tip’.
- Most common obstetric brachial plexus injury.
- Recovery assessed by return of biceps function by 3 months.
Klumpke’s Palsy
- Injury to lower trunk (C8–T1).
- Produces claw hand deformity.
- Weakness of intrinsic hand muscles and wrist flexors.
- Often associated with Horner syndrome.
- Prognosis usually poor.
Total Brachial Plexus Injury
- Involves C5–T1 roots.
- Arm becomes completely flaccid.
- Both motor and sensory loss.
- Has the worst prognosis.
Treatment of Brachial Plexus Injuries
- Initial management: observation and physiotherapy.
- If no recovery (especially biceps function) by 3 months ? suspect root avulsion.
- Surgical options include nerve grafting for postganglionic injuries.
Nerve transfers (neurotization) used for preganglionic injuries


Leave a Reply