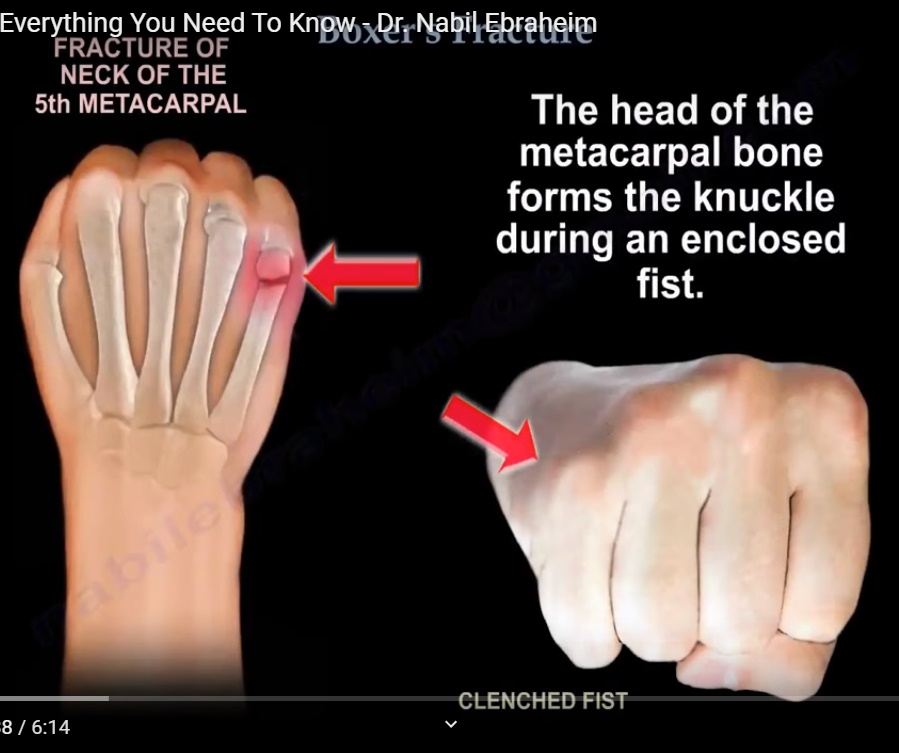
- Fracture of the neck of the fifth metacarpal.
- Most common metacarpal fracture.
- Usually occurs after striking a hard object with a clenched fist.
Mechanism of Injury
Mechanism
- Direct axial load through a clenched fist.
- Commonly occurs after punching a wall or another person.
- Force is transmitted through the fifth metacarpal, causing fracture at its neck.
Pathoanatomy
Fracture pattern
- Fracture usually occurs at the neck of the fifth metacarpal.
- Distal fragment angulates dorsally.
- Metacarpal head displaces palmarly.
- May produce loss of knuckle prominence and pseudo clawing.
Clinical Features
Symptoms
- Pain over the fifth metacarpal.
- Swelling.
- Deformity over the small finger knuckle.
- Tenderness at the fracture site.
Signs
- Dorsal bump.
- Loss of normal knuckle contour.
- Assess carefully for rotational deformity.
Imaging
Radiographs
- Obtain AP, oblique, and true lateral views.
- True lateral view is essential to assess angulation.
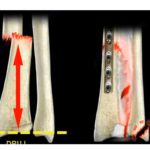
Metacarpal neck angle
- Normal neck angle is approximately 15°.
- Actual deformity = Measured angulation ? 15°.
Carpometacarpal (CMC) Joint Mobility
Second and third CMC joints
- Relatively immobile.
- Deformity is poorly tolerated.
Fourth CMC joint
- Approximately 10 to 15° of compensatory motion.
Fifth CMC joint
- Approximately 20 to 30° of compensatory motion.
- Allows greater acceptance of angulation.
Acceptable Angulation
Fifth metacarpal shaft fracture
- Less than 40° is generally acceptable.
Fifth metacarpal neck fracture
- Less than 50 to 60° of angulation is generally acceptable.
Practical recommendation
- Angulation greater than 50° may require reduction to avoid pseudo clawing.
Treatment
Conservative treatment
- Most fractures are managed nonoperatively.
- Ulnar gutter splint is commonly used.
- Immobilize the hand in the intrinsic plus position.
- Wrist in extension.
- MCP joints flexed.
- Close reduction may be performed if necessary.
Rotational deformity
- Always requires correction.
- Even minimal rotational deformity is poorly tolerated.
Surgical Treatment
Indications
- Significant rotational deformity.
- Unacceptable angulation.
- Unstable fractures.
- Open fractures.
Techniques
- Percutaneous K wire fixation.
- Intramedullary K wire fixation.
- Cross pinning from the fifth to the fourth metacarpal.
Prognosis
Outcome
- Functional outcome is usually excellent.
- Residual dorsal bump is common but rarely affects function.
- Angulation up to 50 to 60° often has satisfactory results.
Recent Evidence
Management
- Studies have shown similar outcomes with buddy taping and splinting for many uncomplicated fractures.
- Pain, grip strength, range of motion, and patient satisfaction are comparable.
- Routine repeated radiographs and prolonged follow up may not always be necessary in uncomplicated cases.
Exam Pearls
Boxer’s fracture
- Fracture of the neck of the fifth metacarpal.
Mechanism
- Punching a hard object with a clenched fist.
Most important deformity
- Rotational deformity must always be corrected.
Acceptable angulation
- Fifth metacarpal neck: up to 50 to 60°.
- Fifth metacarpal shaft: up to 40°.
Immobilization
- Ulnar gutter splint.
- Wrist extended.
- MCP joints flexed.
Reason fifth metacarpal tolerates greater angulation
- Increased mobility of the fifth carpometacarpal joint.


Leave a Reply