Courtesy: Amr Abdelgawad, Maimonaides Medical Centre, Brooklyn, NY, USA
Baker’s Cyst in Children
Introduction
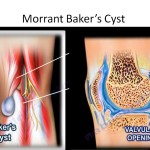
A Baker’s cyst, also known as a popliteal cyst, is a fluid-filled swelling located in the popliteal fossa behind the knee.
In children, Baker’s cysts are generally benign and self-limiting, and they differ significantly from adult Baker’s cysts, which are more commonly associated with intra-articular knee pathology.
Definition
A Baker’s cyst is:
- A fluid-filled cystic swelling in the posterior aspect of the knee
- Typically filled with gelatinous fluid
In children, the cyst most commonly arises between:
- Medial head of gastrocnemius
- Semimembranosus tendon
Epidemiology
Important epidemiological features include:
- More common in boys
- Usually located on the medial side of the popliteal fossa
Most pediatric Baker’s cysts occur without significant underlying joint disease.
Clinical Presentation
Typical Symptoms
Most children present with:
- Painless swelling behind the knee
- Visible bulge in the popliteal region
Associated Features
Some children may experience:
- Mild discomfort after activity
- Sensation of fullness behind the knee
Physical Examination
Typical examination findings include:
- Soft cystic swelling
- Non-tender mass
- No inflammatory signs
The swelling may become more prominent with knee extension.
Natural History
Self-Limiting Condition
Pediatric Baker’s cysts usually resolve spontaneously.
Typical resolution occurs within:
- 6 to 24 months
Most cases require no active intervention.
Imaging
Plain Radiographs
X-rays are typically:
- Normal
Radiographs are mainly used to exclude other pathology.
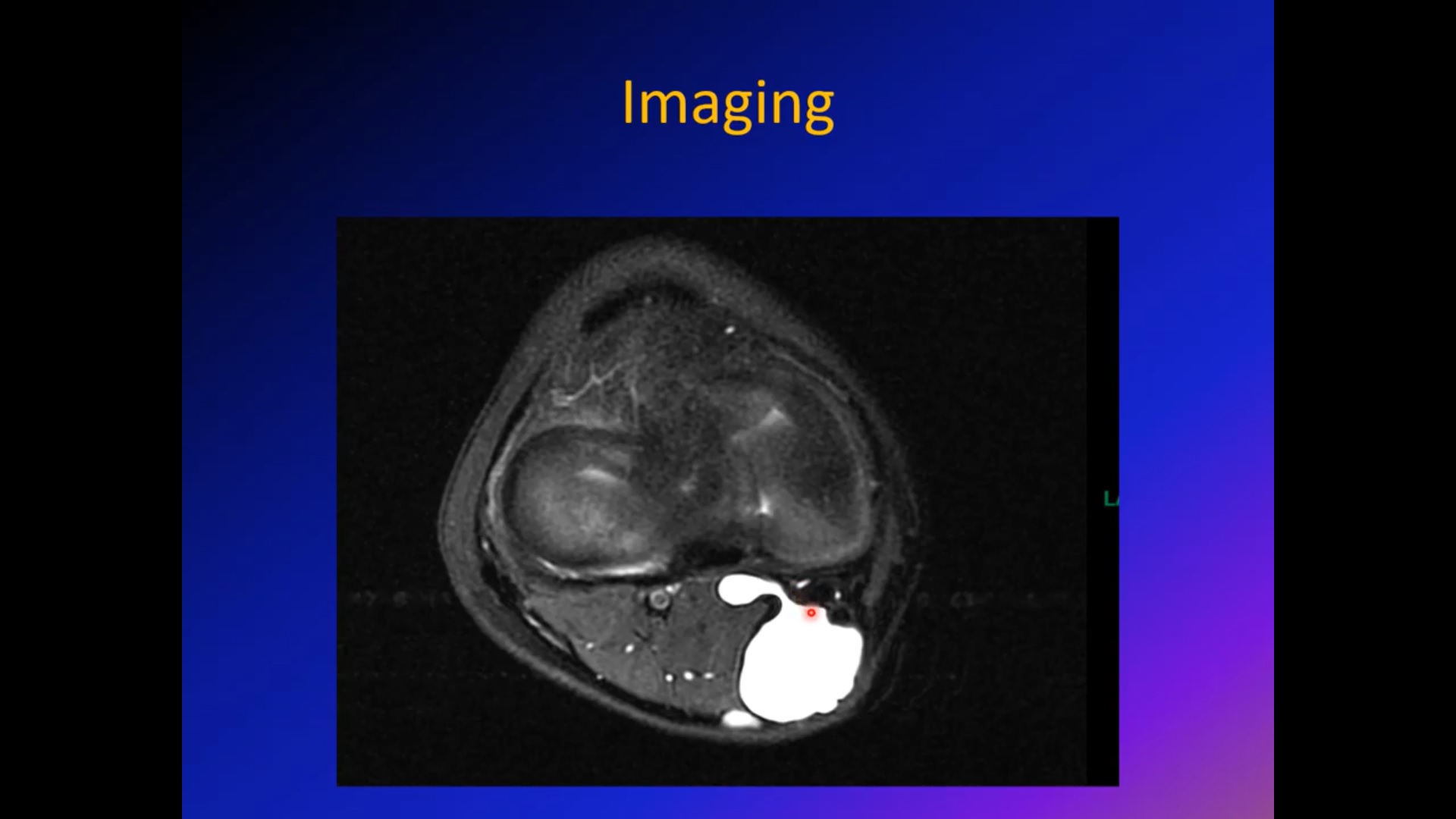
MRI Findings
MRI demonstrates:
- Fluid-filled lesion with high T2 signal intensity
- Typical location between:
- Medial head of gastrocnemius
- Semimembranosus tendon
MRI is generally reserved for atypical or concerning presentations.
Red Flag Features
Certain findings require further evaluation because they may suggest alternative pathology.
Concerning Features
Red flags include:
- Painful swelling
- Rapid enlargement
- Firm or solid mass
- Atypical appearance
- Persistent symptoms
These cases may require advanced imaging and specialist referral.
Differential Diagnosis
Conditions that may mimic a Baker’s cyst include:
- Soft tissue tumors
- Vascular lesions
- Popliteal artery aneurysm
- Synovial pathology
- Ganglion cyst
Careful clinical evaluation is important in atypical cases.
Management
Conservative Treatment
Most pediatric Baker’s cysts are managed non-operatively.
Treatment includes:
- Observation
- Reassurance
- Periodic follow-up
No intervention is required in the majority of patients.
Indications for MRI or Referral
Further evaluation is indicated when there is:
- Increasing cyst size
- Persistent symptoms
- Painful swelling
- Uncertain diagnosis
- Atypical examination findings
Surgical Management
Rarely Required
Surgery is uncommon in children because most cysts resolve spontaneously.
Indications for Surgery
Operative treatment may be considered for:
- Large symptomatic cysts
- Persistent pain
- Functional limitation
- Family preference in selected cases
Surgical Technique
The cyst is typically excised through:
- Posterior approach to the knee
Careful dissection is required to avoid injury to surrounding neurovascular structures.
Prognosis
The prognosis is excellent in most children.
Important points include:
- Most cysts resolve spontaneously
- Long-term complications are rare
- Recurrence after surgery is uncommon but possible
Key Clinical Pearls
- Baker’s cysts in children are usually benign and self-limiting.
- Most present as painless popliteal swellings.
- MRI is reserved for atypical or concerning features.
- Painful or rapidly enlarging masses require further evaluation.
- Surgical treatment is rarely necessary.
- Reassurance and observation are appropriate in most cases.

Leave a Reply