Courtesy – Dr Dinshaw Pardiwala, Dr Ashok Shyam, Ortho TV
Modern Approach to Articular Cartilage Restoration
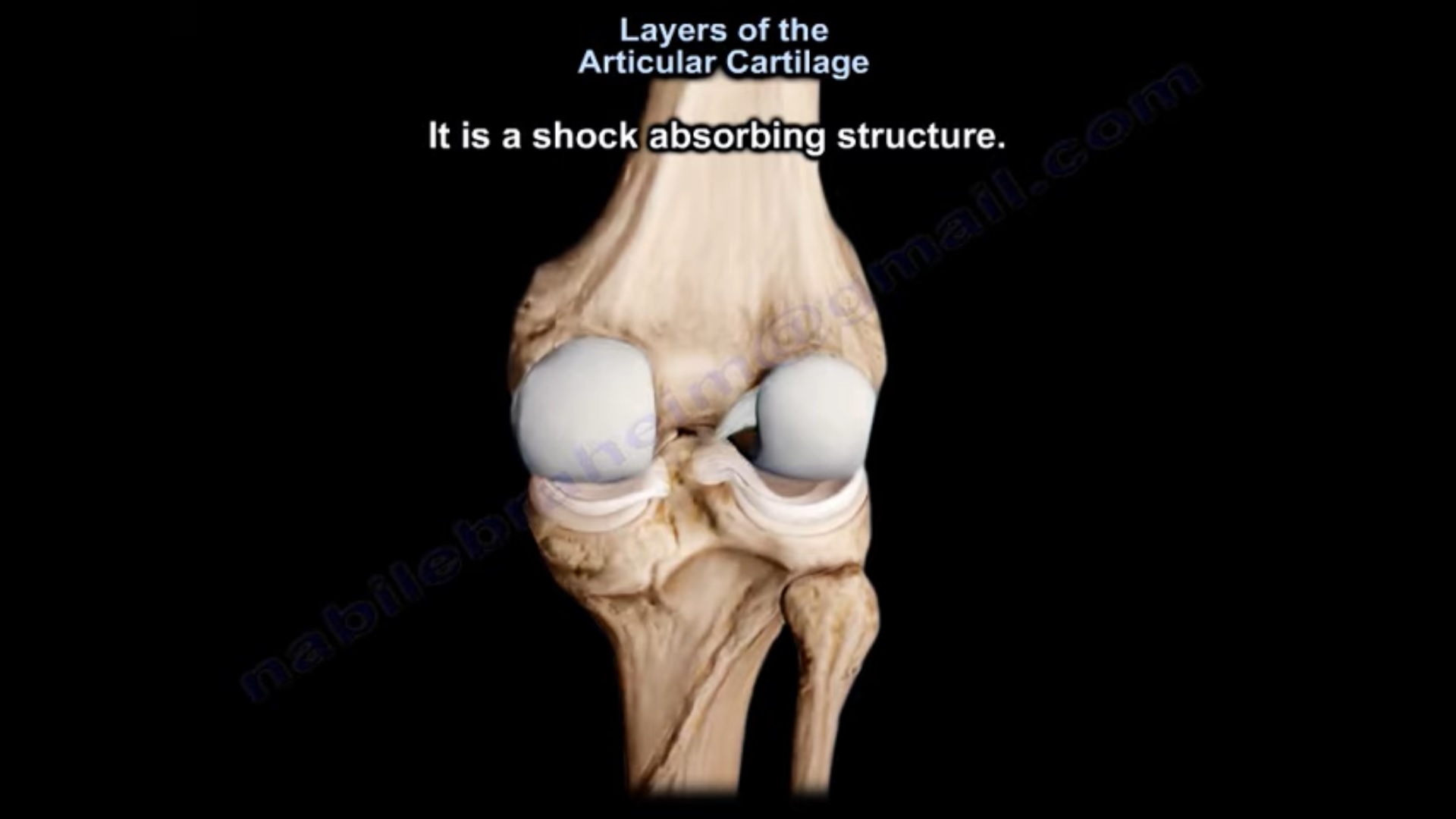
Importance of Articular Cartilage
-
Articular cartilage plays a critical role in knee joint function.
-
It provides a smooth, low-friction surface for joint movement.
-
It helps in even distribution of load across the joint surface.
-
This load distribution reduces peak stresses on the subchondral bone.
Limited Healing Capacity of Cartilage
-
Articular cartilage has very limited ability to heal spontaneously.
-
Full-thickness cartilage defects usually progress over time.
Natural History of Untreated Defects
-
Cartilage defects tend to enlarge progressively.
-
Subchondral bone edema may develop.
-
Over time, degenerative changes appear.
Long-term observations show:
-
Approximately half of patients develop osteoarthritis within fourteen years if defects remain untreated.
Progression of Untreated Cartilage Lesions
Consider a patient with a full-thickness medial femoral condyle cartilage defect.
Initial features:
-
Active middle-aged distance runner
-
Mild varus alignment
-
Continued high load on the joint
Disease Progression
-
Three weeks: localized cartilage defect
-
Three months: enlargement of the lesion
-
Six months: subchondral bone edema appears
-
Five years: early arthritic changes with osteophyte formation
-
Seven years: established medial compartment osteoarthritis
This illustrates the poor prognosis of untreated cartilage lesions.
Surgical Options for Cartilage Restoration
Over the years, several surgical strategies have been developed.
Common options include:
-
Osteochondral fracture fixation
-
Bone marrow stimulation procedures
-
Osteochondral autograft transfer
-
Synthetic plugs
-
Osteochondral allografts
-
Autologous chondrocyte implantation
-
Limited surface replacement implants
Treatment selection depends on lesion characteristics and patient factors.
Management Algorithm for Cartilage Lesions
Treatment decisions are based on:
-
Nature of the lesion
-
Size of the defect
-
Location of the defect
-
Patient age and activity level
-
Associated mechanical factors
Traumatic Osteochondral Fractures
Acute traumatic osteochondral fractures are best treated with fixation.
Surgical Principles
-
Arthroscopic evaluation of the fragment
-
Assessment of subchondral bone viability
-
Anatomical reduction and fixation
Fixation is often performed through a mini-open approach because it allows:
-
Accurate reduction
-
Better control of rotational alignment
Fixation Techniques
Fragments can be fixed using:
-
Countersunk metal screws
-
Bioabsorbable screws
Healing typically occurs through subchondral bone integration.
Management of Delayed Osteochondral Fractures
Delayed presentation does not always preclude fixation.
Research observations have shown:
-
Chondrocytes in osteochondral fragments may remain viable for up to three months.
-
If the cartilage surface appears healthy, fixation may still be successful.
Therefore, even chronic fragments can sometimes be reduced and fixed successfully.
Osteochondritis Dissecans Lesions
For unstable lesions with displaced fragments:
-
Fixation may not always be appropriate.
-
Alternative cartilage restoration procedures may be required.
Partial Thickness Cartilage Defects
Partial thickness defects are commonly treated with chondroplasty.
Indications
-
Symptomatic cartilage flaps
-
Mechanical symptoms such as catching or locking
Surgical Technique
-
Remove unstable cartilage flaps.
-
Smooth and stabilize the surrounding cartilage edges.
Key principle:
-
Avoid aggressive debridement.
-
Preserve as much healthy cartilage as possible.
Full Thickness Cartilage Defects
Full thickness cartilage defects require restorative procedures.
Several surgical options exist.
Bone Marrow Stimulation Techniques
Bone marrow stimulation procedures aim to stimulate cartilage repair.
Technique
-
Remove unstable cartilage edges.
-
Create small perforations in the subchondral bone.
This allows:
-
Bone marrow elements
-
Mesenchymal stem cells
-
Growth factors
to enter the defect and form a fibrocartilage repair tissue.
Technical Considerations
-
Previously, holes were created approximately three millimetres apart.
-
Current understanding suggests that fewer holes may be adequate.
-
Excessive perforation can weaken the subchondral plate.
Limitations
Bone marrow stimulation produces fibrocartilage rather than hyaline cartilage.
Outcomes are variable:
-
Some patients experience excellent results.
-
Others show incomplete or poor cartilage regeneration.
Osteochondral Autograft Transfer
For restoration of hyaline cartilage, osteochondral autograft transfer is often preferred.
This technique is commonly known as mosaicplasty.
Mosaicplasty Technique
-
Osteochondral plugs are harvested from non-weight-bearing areas of the femoral condyle.
-
These plugs are transplanted into the cartilage defect.
The grafts contain:
-
Hyaline cartilage
-
Subchondral bone
This provides a biological restoration of the joint surface.
Indications for Mosaicplasty
Best suited for:
-
Small focal defects
-
Lesions smaller than approximately two square centimetres
Donor Site Considerations
Harvesting multiple grafts increases the risk of:
-
Donor site morbidity
-
Patellofemoral symptoms
Therefore, graft harvesting should be limited.
Technical Challenges
Successful mosaicplasty requires:
-
Accurate perpendicular socket preparation
-
Proper graft sizing
-
Correct depth placement
Important principle:
-
Grafts should not protrude above the articular surface.
Slightly recessed placement is preferable to avoid joint surface irregularity.
Autologous Chondrocyte Implantation
For larger defects, autologous chondrocyte implantation is an important option.
Technique
-
Cartilage biopsy is obtained arthroscopically.
-
Chondrocytes are cultured in a laboratory.
-
Cultured cells are implanted into the defect.
Gel-based implantation systems are widely used in several countries.
Advantages of Autologous Chondrocyte Implantation
This method allows:
-
Restoration of large cartilage defects
-
Reconstruction of complex joint contours
It is particularly useful in areas where shape restoration is critical.
Osteochondral Allograft Transplantation
Osteochondral allografts are used for large structural defects.
Indications
-
Massive osteochondral lesions
-
Failed previous cartilage procedures
-
Segmental condylar defects
Advantages
-
Restoration of both cartilage and subchondral bone
-
Ability to reconstruct large joint surface segments
Limitations
-
High cost
-
Limited availability
-
Need for graft matching
For these reasons, allografts are often reserved for complex cases.
Treatment Based on Lesion Size
A practical treatment strategy can be summarized as follows:
Very Small Lesions
-
Bone marrow stimulation procedures
Small to Medium Lesions
-
Osteochondral autograft transfer
Larger Lesions
-
Autologous chondrocyte implantation
Massive Defects
-
Osteochondral allograft transplantation
Importance of Correcting Predisposing Factors
Cartilage repair will fail if underlying mechanical problems are not addressed.
These include:
-
Limb malalignment
-
Patellofemoral maltracking
-
Ligament instability
Example
In a patient with a cartilage defect and varus alignment:
-
Cartilage repair alone is insufficient.
-
High tibial osteotomy may be required to unload the medial compartment.
Correcting alignment can significantly improve long-term outcomes.
Focal Degenerative Cartilage Defects
A newer option for focal degenerative defects is patient-specific focal resurfacing implants.
Indications for Focal Surface Implants
These implants may be considered in patients with:
-
Localized degenerative cartilage damage
-
Preserved joint alignment
-
Minimal generalized arthritis
Surgical Technique
The procedure involves:
-
Patient-specific implant design based on imaging
-
Creation of a matching socket using custom instrumentation
-
Implant placement slightly recessed below the cartilage surface
Implant Positioning
Implants are usually positioned:
-
Approximately half to one millimetre below the surrounding cartilage.
This prevents the implant from becoming prominent during weight-bearing.
Summary of Treatment Strategy
Management depends on:
-
Lesion size
-
Lesion location
-
Patient characteristics
-
Associated mechanical abnormalities
General principles include:
-
Fix traumatic osteochondral fractures whenever possible.
-
Treat partial thickness lesions with chondroplasty.
-
Select restorative procedures for full thickness defects based on defect size.
-
Correct malalignment or instability when present.
Evolving Perspective on Cartilage Repair
Historically, articular cartilage was believed to have little capacity for repair.
Modern surgical techniques now allow:
-
Restoration of joint surface structure
-
Improved functional outcomes
-
Delay of degenerative arthritis
Advances such as osteochondral transplantation, cell-based therapies, and biological implants have significantly expanded treatment possibilities.

Leave a Reply