Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Overview
Fractures of the radius and ulna shafts require precise surgical exposure to achieve anatomical reduction and stable fixation.
Key Principles
-
Choice of approach depends on fracture location
-
Each approach utilizes specific intermuscular planes
-
Protection of neurovascular structures is critical
Approach to the Ulna Shaft
General Characteristics
-
The ulna is subcutaneous along most of its length
-
Allows direct and straightforward exposure
-
Commonly approached from the dorsal aspect
Surgical Interval
-
Between:
-
Flexor carpi ulnaris (FCU)
-
Extensor carpi ulnaris (ECU)
-
Provides safe access to the ulnar shaft
Structure at Risk
Dorsal Cutaneous Branch of Ulnar Nerve
-
Emerges ~5 cm proximal to the wrist
-
Crosses toward the dorsum of the hand
Must be protected, especially during exposure of the distal ulna
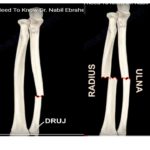
Surgical Approaches to the Radius Shaft
The radius can be exposed via:
-
Volar (anterior) approach
-
Dorsal (posterior) approach
Selection depends on fracture location
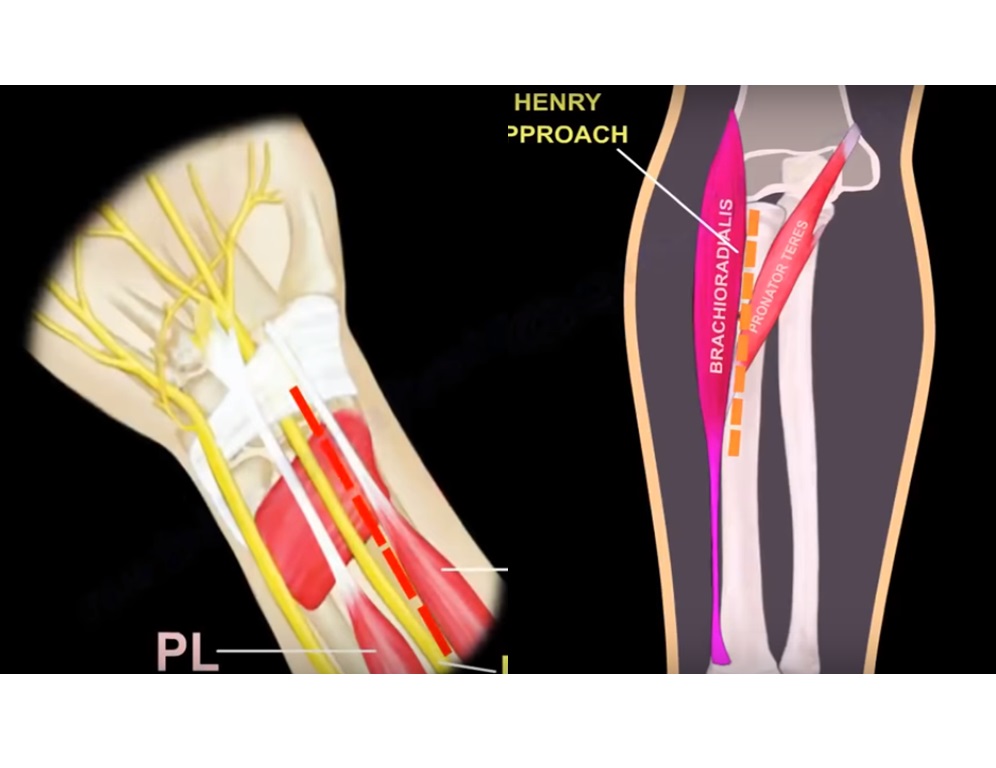
Volar Approach to the Radius
Skin Incision
-
Begins ~1 cm lateral to the biceps tendon insertion
-
Extends distally toward the radial styloid
Intermuscular Planes
Distal Interval
-
Between:
-
Flexor carpi radialis (FCR)
-
Brachioradialis (BR)
-
Proximal Interval
-
Between:
-
Pronator teres (PT)
-
Brachioradialis (BR)
-
Indications
-
Middle third radius fractures
-
Distal third fractures
-
Selected proximal fractures
Structures at Risk
During dissection, protect:
-
Radial artery
-
Superficial radial nerve
-
Palmar cutaneous branch of median nerve
Also consider structures lying beneath retractors
Modified Volar Approach (Distal Consideration)
-
Median nerve lies between:
-
Palmaris longus
-
Flexor carpi radialis
-
Safer Technique
-
Dissect along lateral border of FCR sheath
Reduces risk of median nerve injury
Proximal Extension
-
Maintains interval between:
-
Brachioradialis
-
Pronator teres
-
Structure at Risk
Posterior Interosseous Nerve (PIN)
-
Must be protected during proximal dissection
Dorsal Approach to the Radius
Skin Incision
-
Starts just anterior to the lateral epicondyle
-
Extends distally along the dorsal forearm
Surgical Interval
-
Between:
-
Extensor carpi radialis brevis (ECRB)
-
Extensor digitorum communis (EDC)
-
Deep Dissection
-
The supinator muscle lies deep
-
Must be carefully split to expose the radial shaft
Structure at Risk
Posterior Interosseous Nerve (PIN)
-
Emerges from the supinator muscle
-
Supplies extensor muscles
Must be identified and protected
High-Risk Zone
-
Junction of proximal and middle thirds of radius
Area of greatest vulnerability for PIN injury
Summary of Surgical Intervals
Ulna
-
FCU —} ECU
Radius – Volar Approach
Proximal
-
Brachioradialis — Pronator teres
Distal
-
Brachioradialis — Flexor carpi radialis
Radius – Dorsal Approach
-
ECRB –} EDC
Nerve Supply Patterns of the Forearm
Dorsal Compartment
-
Supplied by:
-
Radial nerve
-
Posterior interosseous nerve (PIN)
-
Volar Compartment
-
Primarily supplied by:
-
Median nerve
-
Important Exceptions
-
Flexor carpi ulnaris (FCU) — Ulnar nerve
-
Ulnar half of flexor digitorum profundus (FDP) — Ulnar nerve
Key Surgical Principle
Volar Approach
-
Typically uses an internervous plane
Between muscles supplied by: -
Median nerve
-
Radial nerve
Dorsal Approach
-
Most muscles share radial nerve supply
Therefore:
-
Greater emphasis on identifying and protecting the posterior interosseous nerve
Key Takeaways
-
Ulna – subcutaneous, easy exposure
-
Radius – requires careful approach selection
-
Volar approach – safer internervous plane
-
Dorsal approach – higher risk to PIN
-
Always identify and protect:
-
Radial artery
-
Median nerve branches
-
Posterior interosseous nerve
-
Leave a Reply