Courtesy Dr Elmar Herbst, Dr Ashok Shyam, Ortho TV
Anterolateral Rotatory Instability (ALRI) of the Knee
Introduction
Anterolateral rotatory instability (ALRI) is a complex instability pattern that commonly occurs following anterior cruciate ligament (ACL) injury. Although ACL reconstruction restores anterior stability in most patients, residual rotational instability may persist despite technically successful surgery. Understanding the biomechanics, anatomy, contributing factors, and treatment options for ALRI is essential for achieving optimal outcomes in ACL reconstruction.
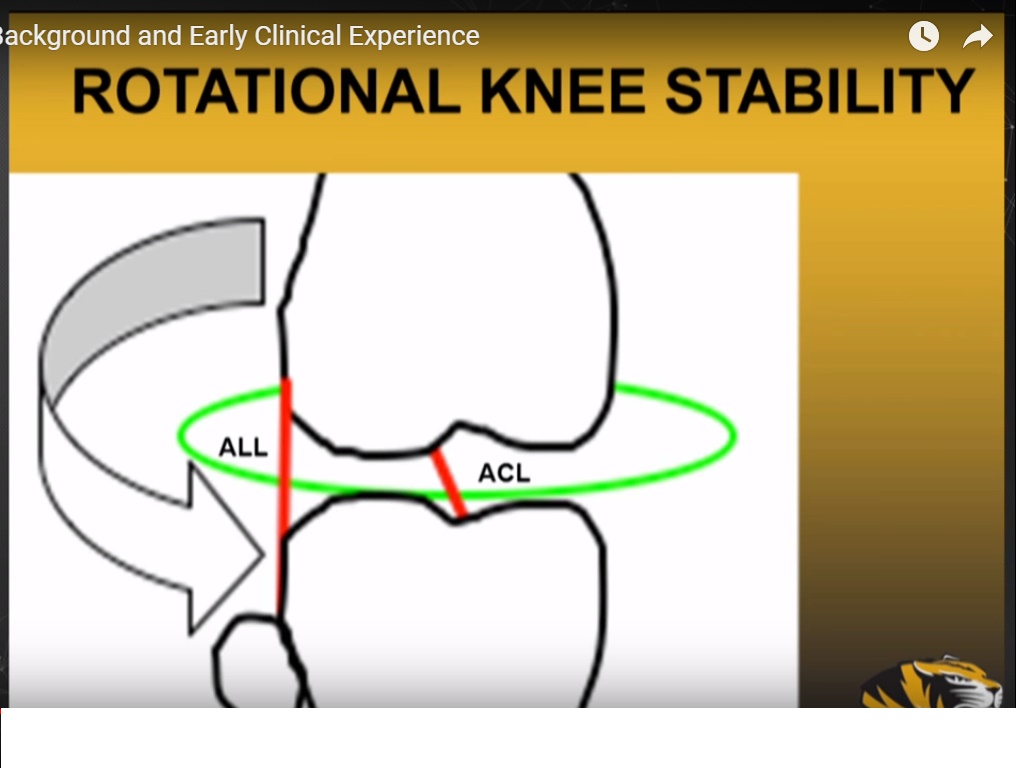
Definition and Biomechanics
Normal Knee Kinematics
In the normal knee:
- The center of rotation lies near the medial tibial spine
- Rotational movement is well controlled by the ACL and surrounding soft tissues
Changes After ACL Injury
After ACL rupture:
- The center of rotation shifts medially
- The lateral compartment demonstrates:
- Increased anterior translation
- Increased internal rotation
These abnormal movements produce anterolateral rotatory instability.
Clinical Assessment
Pivot Shift Test
The pivot shift test is the primary clinical examination used to evaluate ALRI.
Grading
- Grade I — Mild instability
- Grade II — Moderate instability
- Grade III — Severe instability
Not all pivot shifts are identical, and instability patterns vary between patients. Therefore, management should be individualized.
Clinical Significance
Persistent rotational instability following ACL reconstruction is clinically important because it is associated with:
- Poor patient-reported outcomes
- Functional instability
- Increased risk of osteoarthritis
Even after well-performed ACL reconstruction, approximately 10–15% of patients may continue to experience residual instability.
Anatomy of the Anterolateral Complex (ALC)
Evolution of the Concept
Initial attention focused on the anterolateral ligament (ALL). However, current understanding suggests that the ALL is not a distinct and consistently identifiable ligament.
The concept has therefore evolved into the broader anterolateral complex (ALC).
Components of the Anterolateral Complex
The ALC includes:
Iliotibial Band (IT Band)
- Superficial fibers
- Deep fibers (Kaplan fibers)
Capsular Structures
- ALL-like capsular thickening
- Lateral capsule
Meniscocapsular Attachments
- Attachments involving the lateral meniscus
Important Anatomical Insights
Kaplan Fibers
Kaplan fibers, originally described in 1958, are now recognized as important stabilizers of rotational knee stability.
ALL as a Capsular Thickening
The ALL is better understood as part of the capsular complex rather than a separate discrete ligament.
Role of Meniscocapsular Structures
Meniscocapsular attachments contribute significantly to rotational control and pivot shift stability.
Biomechanics of ALRI
Primary and Secondary Restraints
Primary Restraint
- ACL
Secondary Restraints
- Iliotibial band
- Meniscus
- Capsular structures
Among secondary stabilizers, the IT band is considered the most important restraint to rotational instability.
Pivot Shift Mechanics
The pivot shift phenomenon mainly occurs within the first 30–40 degrees of knee flexion.
Contribution of Different Structures
ALL Contribution
- Approximately 10–15%
IT Band Contribution
- Major restraint to rotational instability
Limitations of Cadaveric Studies
Many cadaveric studies remove the IT band during dissection. This may artificially exaggerate the role of the ALL.
In vivo studies demonstrate that the iliotibial band plays the dominant role in controlling rotational stability.
Why ACL Reconstruction May Fail to Restore Normal Kinematics
Non-Anatomic Reconstruction
Improper tunnel placement or non-anatomic reconstruction remains a major cause of persistent ALRI.
Consequences include:
- Increased internal rotation
- Abnormal knee biomechanics
- Residual pivot shift
Causes of Residual Instability
Persistent instability following ACL reconstruction may result from several factors.
1. Missed Secondary Stabilizers
Failure to recognize injury to secondary stabilizers may contribute to ongoing instability.
2. Meniscal Pathology
Particularly important lesions include:
- Posterior root tears
- Lateral meniscal instability
These injuries can significantly increase pivot shift instability.
Clinical Recommendation
Meniscal injuries should always be carefully assessed and repaired whenever possible.
Posterior Tibial Slope
Biomechanical Effect
An increased posterior tibial slope leads to:
- Increased anterior tibial translation
- Greater rotational instability
Management Considerations
In revision ACL cases with excessive slope, slope-reducing osteotomy may be considered.
Bony Factors
Underlying bony deformities may contribute to persistent instability patterns.
These abnormalities cannot be adequately corrected with soft tissue reconstruction alone.
Generalized Ligamentous Laxity
Patients with generalized hyperlaxity have an increased risk of:
- Persistent rotational instability
- Graft failure
- Residual pivot shift
Chronic ACL Deficiency
Long-standing ACL injuries often develop more complex instability patterns due to:
- Secondary soft tissue stretching
- Meniscal damage
- Altered biomechanics
Chronic injuries may therefore require additional stabilization procedures.
Role of Anterolateral Procedures
Types of Procedures
Lateral Extra-Articular Tenodesis (LET)
ALL Reconstruction
Both procedures are designed to augment rotational stability.
Benefits of Anterolateral Augmentation
Studies have demonstrated that adding an anterolateral procedure may:
- Reduce graft failure rates
- Improve rotational stability
- Reduce persistent pivot shift
Reported Failure Rates
- ACL reconstruction alone: approximately 11%
- ACL reconstruction with LET: approximately 4%
The estimated number needed to treat (NNT) is approximately 14 to prevent one graft re-tear.
Risks of Anterolateral Procedures
Potential complications include:
- Over-constraint of the knee
- Increased lateral compartment pressure
- Possible early osteoarthritis
Because of these risks, anterolateral procedures should be used selectively.
Indications for Anterolateral Augmentation
Common indications include:
- Revision ACL reconstruction
- High-grade pivot shift
- Generalized ligamentous laxity
- Young athletes returning to pivoting sports
- High-risk patients
Surgical Principles of LET
Preferred Graft
A strip of iliotibial band is commonly used rather than hamstring grafts.
Technique Overview
The graft is:
- Passed beneath the lateral collateral ligament
- Fixed near the lateral femoral epicondyle
Knee Position During Fixation
- 20–30° knee flexion
- Neutral rotation
Critical Technical Points
Important principles include:
- Avoid overtensioning the graft
- Preserve lateral structures
- Avoid injury to the lateral collateral ligament
Excessive tension may lead to stiffness and over-constraint.
Key Takeaways
- All ACL injuries produce some degree of rotational instability
- Even technically successful ACL reconstruction may not completely restore normal rotational kinematics
- The ALL is not a distinct ligament but part of the broader anterolateral complex
- The iliotibial band is the primary restraint to rotational instability
- Evaluation should always include:
- Meniscal status
- Tibial slope
- Bony alignment
- Generalized laxity
- Anterolateral procedures are valuable in selected patients but should be used carefully to avoid over-constraint


Leave a Reply