Courtesy:Prof Nabile Ebraheim, University of Toledo, Ohio, USA
Anterior Interosseous Nerve (AIN) Syndrome
(Kiloh–Nevin Syndrome)
Introduction
-
Kiloh–Nevin syndrome was first described in 1948 by Parsonage and Turner and later defined in 1952 by Kiloh and Nevin.
-
It represents a compressive forearm neuropathy affecting the anterior interosseous nerve (AIN).
-
Characterized by pure motor deficits without sensory involvement.
-
Also known as Anterior Interosseous Nerve Syndrome.
Origin & Course
-
Motor branch of the median nerve.
-
Arises approximately 4–6 cm distal to the elbow (about one-third down the forearm).
-
Exits from the anterolateral aspect of the median nerve.
-
Travels along the interosseous membrane between the radius and ulna.
-
Lies deep between flexor digitorum profundus (FDP) and flexor pollicis longus (FPL).
-
Accompanies the anterior interosseous artery.
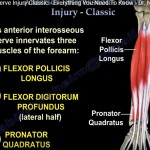
Innervation
-
Purely motor nerve (no cutaneous sensory supply).
-
Supplies three muscles:
-
Flexor Digitorum Profundus (index & middle fingers)
-
Flexor Pollicis Longus
-
Pronator Quadratus
-
-
Terminal branches also supply:
-
Volar wrist capsule
-
Carpal joint capsule
-
Epidemiology
-
Rare condition
-
Accounts for <1% of all median nerve neuropathies
Etiology
Common Sites of AIN Entrapment
-
Tendinous edge of the deep head of pronator teres (most common)
-
Fibrous arch of the flexor digitorum superficialis (FDS)
-
Thrombosed radial, ulnar, or anterior interosseous artery
-
Accessory head of FPL (Gantzer’s muscle)
-
Accessory muscle slips from FDS to FDP
-
Aberrant muscles (e.g., FCR brevis, palmaris profundus)
Causes
-
Idiopathic or spontaneous compression
-
Anatomical variations
-
Trauma (especially supracondylar fractures, usually traction injury)
-
Infections (e.g., CMV)
-
Iatrogenic causes (venipuncture or catheterization in cubital fossa)
-
Compartment syndrome and Volkmann ischemic contracture
Associated Conditions
Parsonage–Turner Syndrome
-
Viral brachial neuritis
-
May cause bilateral AIN palsy
-
Suspected when:
-
Motor weakness follows severe shoulder pain
-
Viral prodrome present
-
Martin–Gruber Anastomosis
-
Communicating branch between median/AIN and ulnar nerve
-
Fibers travel from median nerve across forearm to ulnar nerve
-
Primarily motor fibers
-
Can:
-
Confuse clinical diagnosis
-
Alter EMG interpretation
-
Cause AIN palsy to mimic ulnar nerve dysfunction
-
Clinical Presentation
-
Motor weakness without sensory loss
-
Vague deep forearm pain may be present
-
Pain often absent or short-lived (typically 2–3 weeks)
-
Unlike:
-
Carpal tunnel syndrome
-
Pronator syndrome
-
Physical Examination
Inspection
-
Severe cases may show forearm muscle atrophy
Motor Findings
-
Weak grip and pinch strength
-
Weak flexion of:
-
Thumb
-
Index finger
-
Middle finger
-
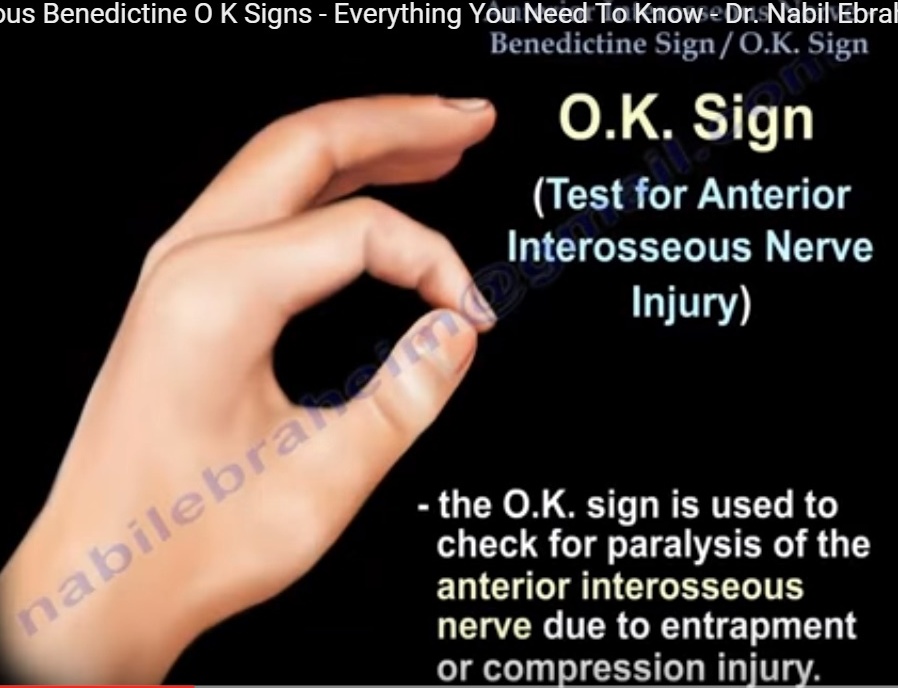
Characteristic Signs
-
Inability to form a proper “OK sign”
-
Also called:
-
Kiloh–Nevin sign
-
Peacock’s eye sign
-
-
Median nerve sensory examination is normal
Provocative & Differentiating Tests
-
Weak resisted pronation with elbow maximally flexed (tests pronator quadratus)
-
Differentiate from FPL tendon rupture:
-
Passive wrist extension should flex thumb IP and index DIP joints (tenodesis effect)
-
Imaging
MRI
Indications
-
Suspected space-occupying lesion
Findings
-
Increased T2/STIR signal in:
-
FPL
-
FDP
-
Pronator quadratus
-
-
Most reliable sign: edema in pronator quadratus
Electrodiagnostic Studies (EMG/NCS)
Role
-
Confirms diagnosis
-
Rules out proximal lesions
-
Assesses severity and recovery
Findings
-
Median nerve conduction: normal
-
Needle EMG:
-
Abnormalities in FPL and FDP (index & middle finger)
-
Fibrillations and sharp waves
-
Prolonged latency
-
Differential Diagnosis
-
Flexor tendon rupture
-
Cervical spine or brachial plexus pathology
-
Pronator syndrome
-
Carpal tunnel syndrome
Key Clinical Distinctions
AIN Syndrome vs Pronator Syndrome
-
AIN: pure motor palsy
-
Pronator syndrome: motor + sensory involvement
AIN Injury vs High Median Nerve Injury
-
AIN Injury
-
Pure motor deficit
-
No sensory loss
-
Cannot form OK sign
-
-
High Median Nerve Injury
-
Motor + sensory loss
-
OK sign deficit with sensory symptoms
-
Important Clinical Signs
OK Sign vs Froment’s Sign
-
OK Sign
-
Tests AIN (FPL + FDP)
-
Flattened pinch instead of circle
-
-
Froment’s Sign
-
Indicates ulnar nerve injury
-
Thumb IP flexes due to FPL compensation
-
Benediction Sign vs Ulnar Claw Hand
-
Benediction Sign
-
Seen in AIN/high median nerve injury
-
Index and middle fingers fail to flex when making a fist
-
-
Ulnar Claw Hand
-
Seen in ulnar nerve injury
-
Ring and little fingers remain flexed on attempted extension
-
Management
Non-Operative (First Line)
-
Observation, rest, and physiotherapy
-
Indicated in absence of space-occupying lesion
-
Most patients improve with conservative care
-
Recovery timeline:
-
Improvement begins: 3–12 months
-
Full recovery: up to 18 months
-
Mean recovery: ~9 months
-
-
Pyridoxine (Vitamin B6) 100 mg for 6–8 weeks may be added
Operative Management
Indications
-
Space-occupying lesion
-
Failure of conservative treatment after 12 months
-
Surgery controversial in patients <40 years, as many recover non-operatively
Outcomes
-
Approximately 75% success rate
Surgical Technique (AIN Decompression)
-
Lazy-S incision over proximal volar forearm
-
Structures released:
-
Lacertus fibrosus
-
Superficial head of pronator teres
-
FDS fibrous arch
-
Gantzer’s muscle (if present)
-
Crossing vessels
-
Any compressive mass
-
-
AIN visualized from proximal to distal
-
Early active motion encouraged post-operatively
Complications
-
Persistent AIN palsy (very rare; 5–10 cases reported)
-
Managed with tendon transfer:
-
Brachioradialis to FPL
-
Prognosis
-
Recovery typically begins 3–12 months after onset
-
Full recovery may take up to 18 months
-
Better prognosis in patients <40 years
Examples of Compression Neuropathies
-
Carpal tunnel syndrome
-
Cubital tunnel syndrome
-
Pronator syndrome
-
Radial tunnel syndrome
-
Posterior interosseous nerve syndrome
-
Tarsal tunnel syndrome
-
Meralgia paresthetica
-
Thoracic outlet syndrome
Leave a Reply