Ankle Fractures – Classification
Overview
- Classification of ankle fractures helps determine:
- Mechanism of injury
- Stability
- Treatment strategy
Two Most Common Systems
- Weber Classification – Based on fracture level
- Lauge-Hansen Classification – Based on mechanism
1. Weber Classification
Principle
- Based on level of fibular fracture relative to:
- Syndesmosis (distal tibiofibular joint)
Weber Type A
- Fracture below syndesmosis
Features
- Usually stable
- Syndesmotic injury uncommon
- Often associated with:
- Supination–adduction injuries
Associated Injuries
- Medial malleolus fracture may be present
Weber Type B
- Fracture at level of syndesmosis
Features
- Most common type
- Stability varies
Associations
- May or may not involve syndesmosis
- Often:
- Supination–external rotation injuries
Weber Type C
- Fracture above syndesmosis
Features
- Usually unstable
- High likelihood of:
- Syndesmotic disruption
- Deltoid ligament injury
Management Note
- Often requires:
- Syndesmotic screw fixation
2. Lauge-Hansen Classification
Principle
- Based on mechanism of injury
Components
1. Foot Position
- Supination
- Pronation
2. Direction of Force
- Adduction
- Abduction
- External rotation
Result
- Combination – 4 injury patterns
Types of Lauge-Hansen Injuries
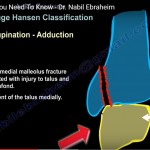
1. Supination–Adduction (SA)
Characteristics
- Vertical medial malleolus fracture
- Transverse distal fibular fracture
- Medial talar displacement
- Anteromedial plafond impaction
Surgical Considerations
- Fixation:
- Parallel lag screws
- Anti-glide plate
Additional Steps
- Elevate impacted plafond
- Restore articular surface
Clinical Note
- Often fix medial side first
2. Supination–External Rotation (SER)
Key Fact
- Most common mechanism
Fibular Fracture Pattern
- Oblique:
- Anterior-inferior – posterior-superior
Stages
- AITFL injury
- Oblique fibular fracture
- Posterior malleolus fracture
- Medial malleolus fracture / deltoid injury
Important Clinical Point
- Always rule out Stage 4 injury
Investigation
- Stress radiographs:
- Detect medial instability
Treatment
- Stage 2 – Conservative
- Stage 4 – Surgical fixation
3. Pronation–External Rotation (PER)
Characteristics
- Injury starts medially
Sequence
- Medial injury
- Syndesmotic injury
- High fibular fracture
- Posterior malleolus involvement
Fibular Fracture
- Above joint level
- Often Weber C equivalent
4. Pronation–Abduction (PA)
Sequence
- Medial malleolus fracture / deltoid injury
- Syndesmotic injury
- Fibular fracture
Fibular Pattern
- Transverse or comminuted
Clinical Note
- May show:
- Syndesmotic injury without fibular fracture
Key Exam Points
- Weber classification – Level of fibular fracture
- Lauge-Hansen classification – Mechanism
High-Yield Facts
- Weber B – Most common fracture type
- SER- Most common mechanism
- SER Stage 4 – Requires surgery
- Weber C – Often needs syndesmotic fixation
Courtesy: Saqib Rehman MD
Associate Professor
Director of Orthopaedic Trauma
Temple Univesity
Philadelphia, Pennsylvania, USA
www.orthoclips.com


Leave a Reply