Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Basic Anatomy of the Talus
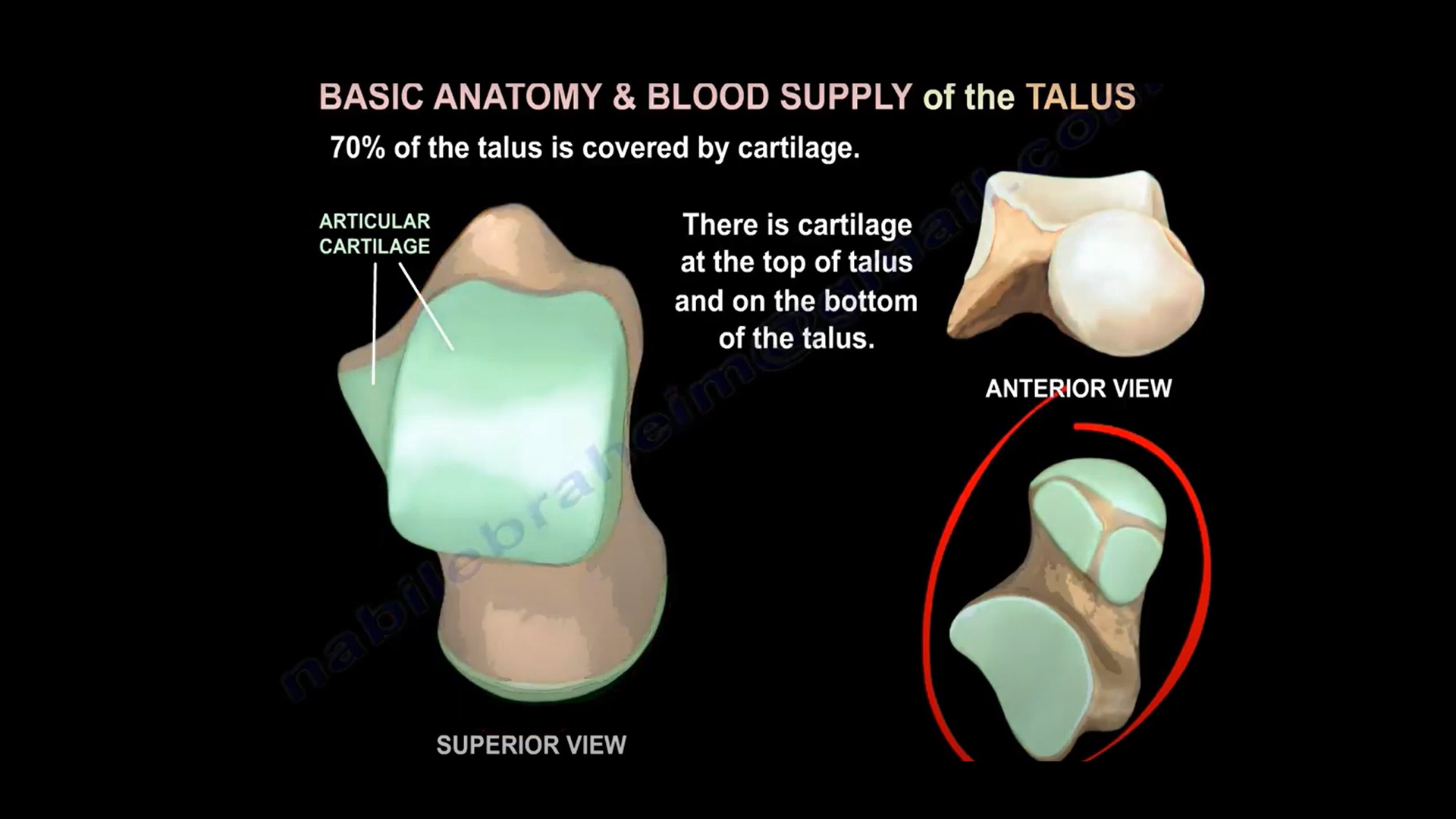
- Approximately 70% of the talus surface is covered by articular cartilage.
- Talus consists of head, neck, body, lateral process, and posterior process.
- Large cartilage coverage contributes to high risk of post?traumatic arthritis after fractures.
Blood Supply of the Talus
- Primary blood supply comes from posterior tibial artery, dorsalis pedis artery, and perforating peroneal artery.
- Medial femoral circumflex equivalent concept does not apply; talus blood supply is relatively tenuous.
- Deltoid branch of the posterior tibial artery may be the only remaining blood supply in severe talar neck fractures.
Important Clinical Point
- Because the talus has limited vascular supply and large cartilage coverage, talar fractures have high risk of avascular necrosis (AVN) and arthritis.
- Subtalar arthritis is the most common complication.
Mechanism of Injury
- Talar neck fractures usually occur due to forceful dorsiflexion combined with axial loading.
- High-energy injuries such as motor vehicle accidents or falls are common causes.
Hawkins Classification of Talar Neck Fractures
- Type I: Non?displaced fracture – AVN risk about 10%.
- Type II: Talar neck fracture with subtalar subluxation or dislocation – AVN risk about 50%.
- Type III: Talar neck fracture with subtalar and tibiotalar dislocation – AVN risk about 90%.
- Type IV: Talar neck fracture with subtalar, tibiotalar, and talonavicular dislocation – AVN risk 90–100%.
Avascular Necrosis (AVN) of the Talus
- Risk correlates strongly with degree of fracture displacement.
- More severe fracture displacement leads to higher risk of AVN.
- AVN may appear as sclerosis on radiographs 3–6 months after injury.
Lateral Process Fracture of the Talus
- Also known as ‘Snowboarder’s fracture’.
- Presents with lateral ankle pain and may be mistaken for ankle sprain.
- CT scan is helpful for diagnosis.
- Non?displaced fractures treated with short leg cast and non?weight bearing for 6 weeks.
- Displaced fractures require surgery.
- Small displaced fragments may be excised.
Types of Lateral Process Fracture
- Type I: Avulsion fracture.
- Type II: Large fragment involving subtalar joint – usually requires surgical fixation.
- Type III: Comminuted fracture – often initially treated with casting.
Posterior Process Fractures
- Posterior process contains medial and lateral tubercles separated by groove for flexor hallucis longus tendon.
- Fracture is rare and frequently missed on initial radiographs.
- May mimic ankle sprain or os trigonum.
Hawkins Sign
- Subchondral radiolucent band seen in talar dome on mortise view at approximately 6–8 weeks after injury.
- Represents subchondral bone resorption due to preserved vascularity.
- Presence of Hawkins sign indicates good talar blood supply and low risk of AVN.
- Absence does not definitively confirm AVN but raises suspicion.
Radiological Evaluation
- Standard radiographs include AP, lateral, and mortise views.
- Canale view is used to visualize talar neck fractures.
- In Canale view: foot pronated 15°, maximally plantarflexed, beam directed 75° cephalad.
- CT scan is very useful for fracture characterization.
- MRI is sensitive for detecting early avascular necrosis.

Leave a Reply