Introduction
-
All-suture (soft) anchors were initially developed for labral repairs and have now gained widespread popularity in rotator cuff repair.
-
Their increasing use is driven by advantages such as:
-
Smaller anchor size
-
Reduced bone footprint occupation
-
Ability to place more fixation points
-
Ease of insertion
-
Ease of revision surgery
-
-
Clinical and biomechanical studies demonstrate that soft anchors perform equivalently to hard-body anchors.
-
Perianchor cyst formation can occur with both soft and hard anchors.
-
A near-vertical angle of insertion is ideal for soft anchor placement.
Evolution of Suture Anchors
-
First generation: Metal anchors
-
Durable but associated with imaging artifacts and difficulty during revision surgery
-
-
Second generation: Polyether ether ketone or poly lactic acid anchors
-
Improved imaging compatibility
-
Bioabsorbable or inert materials
-
-
Third generation: All-suture (soft) anchors
-
Minimal bone footprint
-
Excellent bone preservation
-
Easier revision options
-
Design Characteristics of Soft Anchors
-
Manufactured from:
-
Ultra-high molecular weight polyethylene
-
Braided polyester
-
-
Structural components:
-
Repair sutures enclosed within a textile sheath
-
The sheath expands and anchors within bone
-
-
Deployment mechanism:
-
Pulling the sutures causes the anchor to expand into Y-shaped, V-shaped, or spherical configurations
-
-
Common sizes:
-
Labral repair: 1.3 to 1.8 millimeters
-
Rotator cuff repair: 1.8 to 3.2 millimeters
-
Rationale for Using Soft Anchors in Rotator Cuff Repair
-
Reduced violation of the tendon footprint, creating a better biological healing environment
-
Ability to place more fixation points in a given area, improving:
-
Tendon-bone contact
-
Repair stability
-
-
Faster insertion, especially with self-punching anchor designs
-
Simplified revision surgery:
-
Hard anchors can be placed without removing existing soft anchors
-
-
Less bone damage following anchor pullout compared to hard anchors
Biomechanical Evidence
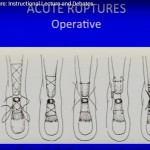
Labral Repair Models
-
Studies demonstrate equivalent load-to-failure values between soft and hard anchors.
-
Mazzocca and colleagues found no difference in failure strength between:
-
2.4-millimeter hard-body anchors
-
1.4-millimeter soft anchors
-
Rotator Cuff Repair Models
-
Soft anchors measuring 1.5 millimeters demonstrated failure strengths exceeding 250 newtons, which is sufficient for rotator cuff repair.
-
Multiple comparative studies show no significant difference in load-to-failure between soft and hard anchors.
-
The Q-Fix soft anchor by Smith & Nephew demonstrated:
-
Similar tensile strength
-
Comparable gap formation when compared with hard anchors
-
Double-Row Repair Biomechanics
-
Studies by Goschka and Bernardoni showed that:
-
Soft anchors in the medial row combined with hard anchors in the lateral row produce biomechanical performance comparable to traditional constructs
-
-
Hoffman and colleagues demonstrated that:
-
Three medial soft anchors produced contact pressures comparable to two medial hard anchors
-
Perianchor Cyst Formation
Experimental and Clinical Evidence
-
Early animal studies, such as those by Pfeiffer and colleagues, showed cavity formation around all-suture anchors, possibly due to micromotion.
-
Perianchor cyst formation has since been observed with:
-
Soft anchors
-
Bioabsorbable anchors
-
Polyether ether ketone anchors
-
-
Clinical studies:
-
Ro and colleagues reported cyst formation in 8.8 percent of soft anchors compared with 16.7 percent of bioabsorbable anchors
-
Kim and colleagues reported no cyst formation with soft anchors at a follow-up of fourteen months
-
Factors Influencing Perianchor Cyst Formation
-
Timing of magnetic resonance imaging:
-
Early imaging (around seven months) may demonstrate more fluid or cyst-like changes
-
These changes often decrease over time
-
-
Angle of anchor insertion:
-
More horizontal insertion angles (approximately sixty-two degrees) are associated with increased cyst formation
-
More vertical insertion angles (approximately sixty-eight degrees or greater) reduce cyst risk
-
Clinical Outcomes
-
Overall clinical outcomes with soft anchors are excellent:
-
High healing rates (approximately seventy-one percent in published series)
-
Significant improvement in pain scores
-
Low retear rates (approximately one to two percent in several studies)
-
-
Anchor settling toward the subchondral bone may occur:
-
This phenomenon has not shown clinical significance to date
-
Importance of Angle of Insertion
-
The traditional “deadman theory” proposed by Burkhart recommended insertion angles less than forty-five degrees for optimal pullout strength.
-
More recent evidence supports a more vertical insertion angle, closer to ninety degrees, especially for soft anchors.
-
Benefits of vertical insertion include:
-
Improved pullout strength
-
Reduced cortical bone damage (minimizing the “windshield-wiper effect”)
-
Lower rates of perianchor cyst formation
-
Reduced retear rates
-
Key Recommendations
-
Aim for a near-vertical anchor insertion angle to improve fixation strength and reduce cyst formation
-
Soft anchors are particularly well suited for medial-row fixation in double-row rotator cuff repairs
-
Bone density should be considered:
-
Anchors may settle deeper in high-density bone
-
Limitations of Current Evidence
-
Limited availability of long-term clinical outcome studies
-
Significant variability in soft anchor design, meaning not all anchors perform identically
Conclusion
-
Soft anchors are biomechanically and clinically non-inferior to hard-body anchors.
-
Key advantages include:
-
Preservation of bone stock
-
Ease of revision surgery
-
Ability to place multiple fixation points
-
-
Current evidence suggests that concerns regarding perianchor cyst formation are largely not clinically significant.
-
Surgical technique, particularly anchor insertion angle, plays a critical role in optimizing outcomes.
It seems Suture anchor you use for tendo achiilis repair is unloaded. Please explain
2/4 of my anchors backed out , one 4 months post op and the other 2 years post op. Is this normal ?