Introduction
-
Scoliosis is defined as an abnormal coronal plane curvature of the spine, usually appearing as a C-shaped or S-shaped curve.
-
A spinal curve measuring greater than ten degrees is considered scoliosis.
-
Hippocrates (four hundred sixty to three hundred seventy-seven before Christ) was the first to describe abnormal spinal curvature and coined the term scoliosis, derived from the Greek word skolios, meaning crooked.
-
Claudius Galen (one hundred thirty-one to two hundred one after Christ) classified spinal deformities into scoliosis, kyphosis, and lordosis.
-
The Growing Spine Study Group and the Children Spine Study Group define early onset scoliosis as any spinal deformity present before ten years of age, regardless of cause.
-
Adolescent idiopathic scoliosis refers to abnormal spinal curvature developing during the growth spurt between ten and eighteen years of age.
Idiopathic Scoliosis
-
Idiopathic scoliosis has no identifiable cause and is not associated with other systemic diseases.
-
Subtypes according to the Scoliosis Research Society:
-
Infantile idiopathic scoliosis: younger than three years
-
Juvenile idiopathic scoliosis: four to ten years
-
Adolescent idiopathic scoliosis: ten to eighteen years
-
-
Curve severity:
-
Mild: less than twenty-five degrees
-
Moderate: twenty-five to fifty degrees
-
Severe: greater than fifty degrees
-
Epidemiology and Demographics
-
Most common form of scoliosis.
-
Positive family history is frequently present.
-
Affects up to four percent of adolescents.
-
Incidence:
-
Curves between ten and twenty degrees: approximately three percent
-
Curves greater than thirty degrees: approximately zero point three percent
-
-
Sex distribution:
-
Small curves: equal male to female ratio
-
Curves greater than thirty degrees: female predominance of approximately ten to one
-
-
Curve patterns:
-
Thoracic curves are more common than lumbar curves
-
Most common pattern is a right thoracic curve
-
Pathophysiology
-
Exact cause remains unknown.
-
Proposed contributing factors include:
-
Genetic influences
-
Neurological factors
-
Hormonal and metabolic abnormalities
-
Skeletal growth imbalance
-
Biomechanical forces
-
Environmental and lifestyle factors
-
Clinical Presentation and Examination
History
-
Age at first detection of deformity
-
Rate and pattern of progression
-
Perinatal and developmental history
-
Family history of scoliosis
-
Menstrual history in female patients
Clinical Presentation
-
Commonly detected due to cosmetic concerns raised by parents
-
Often identified during school screening programs
-
A scoliometer reading greater than seven degrees during the Adams forward bending test correlates with a coronal plane curve of approximately twenty degrees
-
Typically painless
-
Neurological symptoms are uncommon
Physical Examination
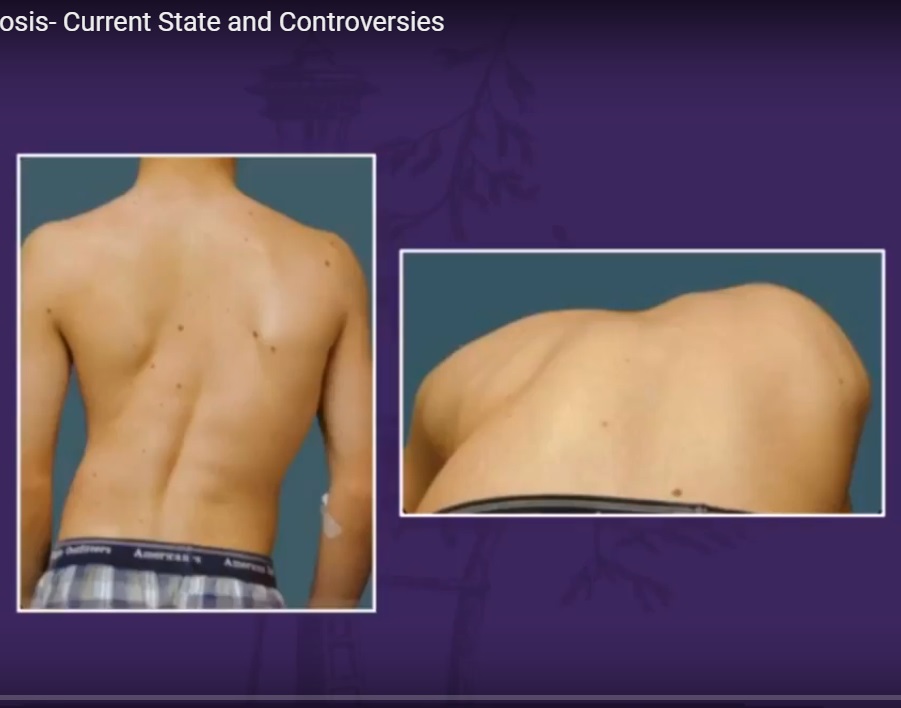
General Inspection
-
Shoulder asymmetry or scapular prominence
-
Deviation of the spine from the midline
-
Head not centered over the pelvis
-
Rib or lumbar prominence on one side
-
Pelvic asymmetry and uneven waistline
-
Asymmetric skin creases
-
Inability to stand erect without compensation
Associated Findings
-
Café-au-lait spots suggesting neurofibromatosis
-
Nevi
-
Cavovarus foot deformities suggesting neural axis abnormalities and warranting magnetic resonance imaging
-
Serial height measurements to identify peak height velocity
-
Limb length discrepancy causing compensatory scoliosis
Spine Examination
-
Midline skin abnormalities such as dimples or hairy patches suggesting spinal dysraphism
-
Rib rotational deformity
-
Adams forward bending test to assess structural curves
-
Sitting forward bending test to exclude limb length discrepancy
Neurological Examination
-
Motor and sensory assessment
-
Deep tendon reflexes
-
Abdominal reflexes
-
Assessment for clonus, Hoffmann sign, and Babinski response
-
Gait analysis
Adams Forward Bending Test
-
Most reliable clinical screening test for scoliosis
-
Patient bends forward with arms hanging freely
-
Symmetry of the trunk is assessed
-
Rib or lumbar hump suggests structural scoliosis
-
Scoliometer may be used to measure trunk rotation
-
Trunk rotation less than seven degrees is considered normal
Curve Progression
Risk Factors
-
Curve magnitude at presentation
-
Curve pattern
-
Remaining skeletal growth
Assessment of Skeletal Maturity
-
Tanner staging
-
Risser staging
Risser Staging
-
Assesses remaining growth potential using pelvic radiographs
-
Based on ossification of the iliac apophysis from lateral to medial
Stages:
-
Risser zero: no ossification, significant growth remaining
-
Risser one: up to twenty-five percent ossification
-
Risser two to four: progressive ossification
-
Risser five: skeletal maturity
Natural History After Maturity
-
Thoracic curves greater than fifty degrees progress one to two degrees per year
-
Lumbar curves greater than forty degrees progress one to two degrees per year
Imaging: Radiographs
-
Standing posteroanterior and lateral radiographs recommended
-
Images should include the iliac crest distally and cervical spine proximally
-
Supine side-bending radiographs used for surgical planning
-
Radiographic assessment includes:
-
Cobb angle
-
Apical vertebra
-
End vertebrae
-
Neutral vertebrae
-
Stable vertebra
-
Curve location and direction
-
Risser sign
-
Radiographic Parameters
Cobb Angle
-
Scoliosis defined as curvature greater than ten degrees
-
Measurement error ranges from three to five degrees
Spinal Balance
-
Coronal balance assessed by alignment of the seventh cervical vertebra plumb line with the central sacral vertical line
-
Sagittal balance assessed by the relationship of the seventh cervical vertebra to the posterior superior corner of the first sacral vertebra
Clavicle Angle
-
Best predictor of postoperative shoulder balance
Vertebral Definitions
-
Apical vertebra: most laterally deviated and rotated vertebra
-
End vertebrae: most tilted vertebrae at the upper and lower ends of the curve
-
Neutral vertebra: first vertebra without rotation above and below the apex
-
Stable vertebra: vertebra most closely bisected by the central sacral vertical line
Vertebral Rotation: Nash–Moe Method
-
Estimates vertebral rotation based on pedicle displacement
-
Grades range from zero to four
-
Advantages:
-
Simple and reproducible
-
-
Limitations:
-
Provides only an approximate estimate of rotation
-
Imaging: Magnetic Resonance Imaging
-
Imaging extends from posterior cranial fossa to conus medullaris
-
Used to detect intraspinal abnormalities
-
Indications include:
-
Left thoracic curve
-
Rapid progression
-
Excessive kyphosis
-
Neurological symptoms
-
Structural abnormalities
-
Foot deformities
-
Asymmetric abdominal reflexes
-
Classification Systems
-
Schulthess classification
-
Ponseti and Friedman classification
-
King–Moe classification
-
Lenke Classification (most widely used)
Lenke Classification System
-
Developed to overcome limitations of earlier systems
-
Uses standing, lateral, and bending radiographs
-
Three-step approach:
-
Identification of primary curve
-
Lumbar modifier determination
-
Thoracic sagittal modifier assignment
-
-
Defines forty-two distinct curve patterns
-
Guides surgical fusion levels
Management Considerations
-
Remaining growth potential
-
Curve magnitude
-
Curve pattern
-
Sex
-
Genetic risk profiling
Non-Surgical Management
Observation
-
Indicated for curves less than twenty-five degrees
-
Serial radiographic monitoring:
-
Mild curves: every six to twelve months
-
Moderate curves: every four to six months
-
Bracing
-
Indicated for progressive curves between twenty-five and forty degrees in skeletally immature patients
-
Full-time or part-time wear depending on curve and compliance
-
Common orthoses:
-
Cervicothoracolumbosacral orthosis
-
Thoracolumbosacral orthosis
-
Night-time bending braces
-
-
Successful bracing reduces surgical requirement by approximately fifty percent
Surgical Management
Goals of Surgery
-
Correct deformity
-
Maintain coronal and sagittal balance
-
Preserve pulmonary function
-
Minimize pain and morbidity
-
Optimize long-term function
Indications
-
Progressive curves greater than forty degrees in skeletally immature patients
-
Curves greater than fifty degrees in skeletally mature patients
Surgical Techniques
-
Posterior spinal instrumentation and fusion (most common)
-
Anterior spinal instrumentation and fusion
-
Combined anterior and posterior fusion for severe or rigid curves
Complications
-
Neurological injury (approximately one in one thousand)
-
Excessive blood loss
-
Pseudarthrosis
-
Superior mesenteric artery syndrome
-
Implant-related complications
-
Infection, often presenting late
-
Flat back syndrome
-
Crankshaft phenomenon in immature patients
Conclusion
-
Adolescent idiopathic scoliosis is a complex three-dimensional spinal deformity.
-
Early detection, accurate assessment, and individualized management are essential.
-
Advances in classification, bracing, and surgical techniques have significantly improved outcomes.
-
Long-term success depends on appropriate patient selection, meticulous technique, and structured follow-up.
Leave a Reply