Definition
-
Acromioclavicular joint separations are disruptions of the acromioclavicular joint complex.
-
Injuries often involve both:
-
Acromioclavicular ligaments
-
Coracoclavicular ligaments
-
Epidemiology
-
Common in young and active adults.
-
Frequently seen in athletes.
-
High incidence in individuals exposed to direct shoulder trauma such as cyclists and football players.
Mechanism of Injury
-
Most commonly caused by:
-
Direct blow to the lateral aspect of the shoulder
-
Fall onto an adducted arm
-
-
Results in superior displacement of the clavicle relative to the acromion.
Classification
-
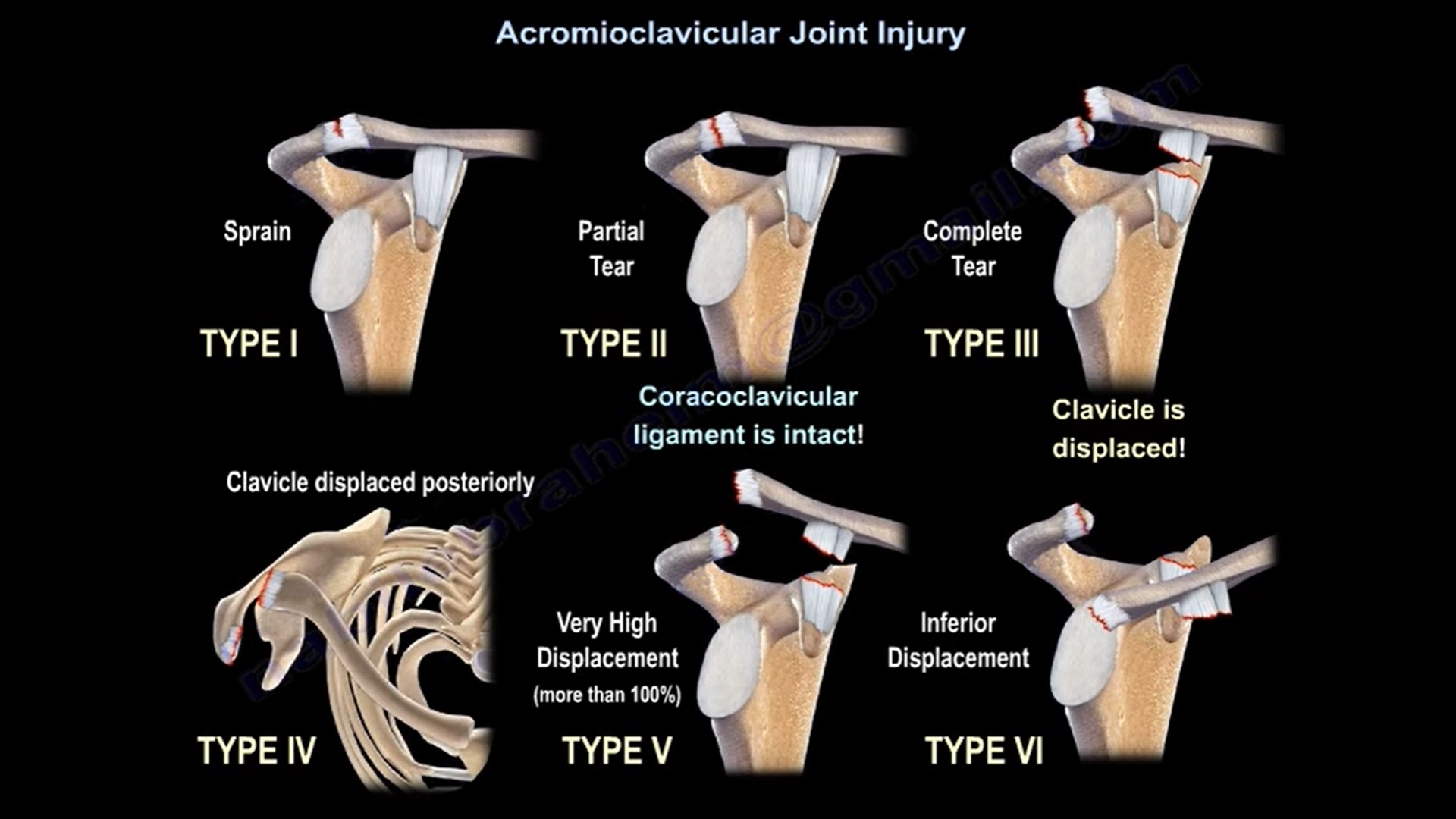
Rockwood classification (Types I to VI)
- Type I: Sprain of the AC ligament. Normal radiograph
- Type II: AC ligament tear, coracoclavicular ligaments sprained. Radiograph demonstrates AC joint widening (normal AC joint distance is 1 to 3mm). Stress views show identical coracoclavicular distance compared to uninvolved side
- Type III: AC and coracoclavicular ligament torn. Radiograph demonstrates loss of AC joint relationship and increased coracoclavicular distance in stress view (25% to 100% greater than the normal side.).
- Type IV: Type III with distal clavicle displaced posteriorly into or through the trapezius
- Type V: Type III with the distal clavicle grossly displaced superiorly.
- Type VI: AC dislocated with the clavicle displaced inferior to the acromion or the coracoid.
Surgical Options Overview
-
Coracoclavicular screw fixation
-
Kirschner wire fixation
-
Hook plate fixation
-
Suspensory fixation systems
-
Graft-based reconstructions using autograft, allograft, or synthetic materials
Coracoclavicular Screw Fixation
Concept
-
Restores joint stability by reducing the coracoclavicular interval using a screw between the clavicle and coracoid.
Biomechanics
-
Provides rigid fixation by transmitting load through the screw, indirectly stabilizing the conoid and trapezoid ligaments.
Technique
-
A 4.5 millimeter cortical or lag screw is placed between the coracoid base and inferior clavicle.
-
Fixation is maintained until ligament healing occurs.
Advantages
-
Technically simple and reproducible
-
Cost-effective
-
Provides immediate stability
Limitations
-
Excessive rigidity limits physiologic micromotion required for ligament healing
-
Requires routine implant removal
Complications
-
Screw loosening, breakage, or pull-out
-
Loss of reduction due to implant failure or early loading
-
Soft tissue irritation from prominent screw head
-
Recurrent dislocation rates higher than suspensory fixation
Prevention Strategies
-
Use partially threaded 4.5 millimeter screws with washers
-
Avoid over-compression
-
Plan implant removal at 8 to 12 weeks
-
Avoid use in overhead athletes
Kirschner Wire Fixation
Concept
-
Transarticular wires stabilize the acromioclavicular joint temporarily.
Technique
-
Two wires placed across the joint under imaging guidance.
-
Often combined with coracoclavicular ligament repair.
Advantages
-
Simple and cost-efficient
-
Provides short-term stability in acute injuries
Complications
-
Wire migration into thorax or mediastinum
-
Wire breakage or loosening
-
Loss of reduction
-
Pin tract infection
-
Recurrent instability after wire removal
Prevention Strategies
-
Use thick wires of at least 2 millimeters
-
Bend wire ends externally
-
Remove wires at 6 weeks
-
Always combine with soft tissue or ligament augmentation
-
Avoid in osteoporotic bone
Hook Plate Fixation
Concept
-
A contoured plate with a hook placed beneath the acromion to restore alignment.
Biomechanics
-
Acts as a lever to maintain reduction and allow early motion.
Technique
-
Plate fixed to lateral clavicle with the hook engaging beneath the acromion.
-
Implant removed after ligament healing, usually at 3 to 4 months.
Advantages
-
Strong fixation
-
Allows early postoperative range of motion
-
Provides reliable vertical stability
Complications
-
Loss of reduction
-
Subacromial impingement and acromial erosion
-
Rotator cuff irritation
-
Mandatory second surgery for implant removal
Risk Factors for Failure
-
Female sex
-
Surgery delayed beyond 7 days
-
Coracoclavicular displacement ratio greater than 1.5
Prevention Strategies
-
Ensure proper hook depth and plate contouring
-
Use hook angles between 0 and 40 degrees
-
Timely implant removal
Suspensory Fixation Systems
Concept
-
Uses cortical buttons and high-strength sutures to recreate coracoclavicular ligament function while allowing controlled micromotion.
Biomechanics
-
Semi-rigid fixation resists superior translation while permitting physiologic movement.
Key Surgical Steps
-
Achieve anatomic reduction
-
Protect neurovascular structures
-
Drill clavicular tunnel and deploy button beneath coracoid
-
Restore coracoclavicular distance
-
Augment with graft when required
Technical Variations
-
Single clavicular tunnel
-
Double clavicular tunnels for anatomic reconstruction
-
Tunnel-free loop-around techniques
-
Hybrid constructs combining suspensory fixation and graft
Complications
-
Coracoid fracture, especially with multiple or large tunnels
Prevention Strategies
-
Use central tunnels and dual-button constructs
-
Avoid multiple coracoid tunnels
-
Use tunnel-free techniques in fragile bone
-
Follow protected rehabilitation for 6 weeks
Graft-Based Reconstructions
Concept
-
Biological reconstruction of coracoclavicular ligaments using tendon grafts.
-
Ideal for chronic injuries or failed previous fixation.
Types
-
Weaver–Dunn procedure
-
Modified Weaver–Dunn procedure
-
Anatomic coracoclavicular ligament reconstruction
Graft Options
-
Autograft: semitendinosus or gracilis
-
Allograft: Achilles or tibialis tendon
-
Synthetic grafts
Advantages
-
Restores vertical and horizontal stability
-
Promotes biological healing
-
No routine implant removal
Complications
-
Loss of reduction due to graft stretching
-
Clavicle or coracoid fracture
-
Tunnel widening
-
Graft rupture or elongation
-
Foreign body reaction with synthetic grafts
Prevention Strategies
-
Prefer autograft for biological incorporation
-
Restore native coracoclavicular distance of approximately 11 to 13 millimeters
-
Combine with suspensory fixation for early stability
-
Use tunnel-free techniques in small coracoids
Persistent Horizontal Instability
Definition
-
Residual anteroposterior instability despite restoration of vertical alignment.
Cause
-
Inadequate repair of acromioclavicular capsule and deltotrapezial fascia.
Incidence
-
Reported in up to 40 percent after isolated coracoclavicular fixation.
Clinical Features
-
Pain with cross-body adduction
-
Mechanical clicking
-
Prominent distal clavicle
-
Functional limitation
Prevention
-
Repair acromioclavicular capsule
-
Add horizontal stabilization techniques
-
Ensure proper clavicle positioning
-
Meticulous deltotrapezial fascia closure
Peri-Implant Fractures
Common Sites
-
Clavicle
-
Coracoid
-
Acromion
Risk Factors
-
Multiple tunnels
-
Large drill diameters
-
Eccentric tunnel placement
-
Early aggressive rehabilitation
-
Poor bone quality
Common Causes of Failure
-
Implant failure or migration
-
Graft elongation or rupture
-
Malpositioned tunnels
-
Excessive or insufficient tension
-
Premature return to activity
Prevention
-
Achieve anatomic reduction
-
Maintain physiologic tension
-
Use combined fixation strategies
-
Delay return to contact sports until healing confirmed
Nonsurgical Management
Indications
-
Rockwood Type I injuries
-
Rockwood Type II injuries
-
Selected Rockwood Type III injuries in low-demand patients
Treatment Phases
-
Immobilization phase: 0 to 3 weeks
-
Rehabilitation phase: 3 to 6 weeks
-
Return-to-activity phase: 6 to 12 weeks
Limitations
-
Possible persistent pain or weakness
-
Cosmetic deformity
-
Risk of chronic instability or degenerative changes
Summary
-
Acromioclavicular joint separations require treatment tailored to injury severity and patient demands.
-
Numerous fixation techniques exist, each with specific advantages and complications.
-
Loss of reduction and peri-implant fractures are the most common complications.
-
Suspensory fixation and anatomic graft reconstructions provide superior biomechanical stability.
-
Rigid fixation methods have higher complication rates and often require implant removal.
-
Addressing horizontal instability and meticulous surgical technique are essential for optimal outcomes.
-
Nonsurgical management remains effective for selected low-grade injuries when combined with structured rehabilitation.

Leave a Reply