Courtesy: Manuel Santos Carvalho MD, Porto, Portugal
Anatomy
-
The Achilles tendon is the largest and strongest tendon in the human body.
-
It is formed by the confluence of the gastrocnemius and soleus tendons.
-
The soleus contribution is relatively short, ranging from 3 to 11 centimeters.
-
The gastrocnemius contributes the major portion, ranging from 11 to 26 centimeters.
-
The tendon inserts on the posterior aspect of the calcaneus, inferior to the superior calcaneal tuberosity.
-
During its course, the tendon undergoes approximately 90 degrees of rotation:
-
The gastrocnemius component attaches laterally.
-
The soleus component attaches medially.
-
-
The tendon is protected from friction by:
-
The retrocalcaneal bursa
-
The posterior subcutaneous calcaneal bursa
-
-
Blood supply is derived primarily from branches of the posterior tibial artery.
Physiology
-
The Achilles tendon demonstrates a remarkable adaptive response to mechanical stress.
-
Regular exercise leads to an increase in tendon diameter and strength.
-
Prolonged inactivity results in rapid tendon atrophy.
-
With increasing age, there is a reduction in cellularity and collagen content.
-
A hypovascular “watershed” zone is present 3 to 6 centimeters proximal to the calcaneal insertion, which is the most common site of rupture.
Function
-
Primary function is plantar flexion of the foot.
-
Plays a crucial role in human locomotion and propulsion.
-
Essential for walking, running, and jumping.
-
The Achilles tendon is subjected to tensile loads of up to 10 times body weight during activity.
Blood Supply
-
Posterior tibial artery supplies the proximal and distal portions of the tendon.
-
Peroneal artery supplies the midportion, including the watershed area.
Innervation
-
Sural nerve is the primary sensory nerve in close relation to the tendon.
-
Tibial nerve provides motor innervation to the gastrocnemius-soleus complex.
Tendoachilles Rupture: Epidemiology
-
Commonly seen in young athletes and individuals involved in recreational sports.
-
More frequent in males.
-
Most commonly occurs between 30 and 40 years of age.
-
Often associated with sudden high-energy movements during sports.
Risk Factors
-
Episodic athletic activity, commonly described as the “weekend warrior” phenomenon.
-
Local corticosteroid injections.
-
Degenerative tendon changes associated with aging.
Mechanism of Injury
-
Most commonly a traumatic injury sustained during sporting activities.
-
Typical mechanism is sudden dorsiflexion of a plantar-flexed foot.
-
Rupture usually occurs 4 to 6 centimeters proximal to the calcaneal insertion in the hypovascular region.
-
Direct trauma from a sharp or angular object can cause rupture at any level of the tendon.
Clinical Presentation
-
Sudden onset of pain in the posterior ankle region.
-
Sensation of a snap or “pop” at the time of injury.
-
Immediate difficulty or inability to walk.
-
Rapid onset swelling around the ankle.
-
History of preceding minor trauma or tendon discomfort may be present.
Clinical Examination
-
Increased resting ankle dorsiflexion when examined prone with knees flexed.
-
Palpable gap or irregularity along the course of the tendon.
-
Inability to perform toe walking.
-
Thompson (Simmonds) test:
-
Absence of plantar flexion when the calf is squeezed indicates rupture.
-
-
O’Brien needle test:
-
Cranial movement of the needle tip on dorsiflexion suggests tendon continuity.
-
-
Copeland test:
-
A sphygmomanometer cuff inflated to 100 millimeters of mercury around the calf.
-
Dorsiflexion increasing pressure to 140 millimeters of mercury suggests an intact tendon.
-
Investigations
-
Radiographs
-
Lateral ankle radiograph may demonstrate Toygar’s sign, based on the posterior skin contour angle.
-
-
Ultrasonography
-
Investigation of choice.
-
Demonstrates tendon discontinuity, edema, hematoma, fibrosis, and tenosynovitis.
-
Useful in differentiating complete and partial ruptures and measuring tendon gap.
-
-
Magnetic Resonance Imaging
-
Reserved for chronic ruptures, equivocal ultrasonography, or suspected infection.
-
Treatment
Conservative Management
-
Functional bracing or casting with the ankle in resting equinus.
-
Suitable for:
-
Acute injuries
-
Low-demand or sedentary patients
-
Medically frail patients
-
Patient or surgeon preference for nonoperative care
-
-
Preferred when:
-
Tendon gap is less than 5 millimeters on ultrasonography
-
Gap is less than 10 millimeters in neutral position
-
Adequate tendon apposition is present
-
-
Outcomes:
-
Comparable plantar flexion strength to operative management
-
Similar re-rupture rates when early functional rehabilitation is used
-
Lower complication rates compared to surgery
-
Surgical Management
-
Open end-to-end Achilles tendon repair is the standard approach.
-
Indicated in:
-
Acute ruptures
-
Young, active individuals
-
High functional demand patients
-
Chronic Tendoachilles Rupture
-
Defined as rupture presenting more than 6 weeks after injury.
-
Presentation includes:
-
Weakness of ankle plantar flexion
-
Difficulty with push-off during gait
-
-
Pathophysiology:
-
Fibrous tissue formation
-
Tendon elongation
-
Possible hypertrophy of the plantaris tendon
-
-
Thompson test may be falsely negative due to fibrous continuity.
Classification and Reconstruction
-
Myerson Classification
-
Type 1 defect (1–2 centimeters): End-to-end repair
-
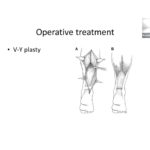
Type 2 defect (2–5 centimeters): V–Y lengthening with or without tendon transfer
-
Type 3 defect (greater than 5 centimeters): Tendon transfer with or without V–Y advancement
-
Reconstructive Techniques
-
V–Y advancement:
-
V-shaped incision with apex at the musculotendinous junction
-
Incision through superficial tendon fibers, preserving muscle
-
-
Tendon transfers:
-
Flexor hallucis longus (most commonly used)
-
Flexor digitorum longus
-
Peroneus longus
-
-
Flexor hallucis longus transfer:
-
Performed through the same incision
-
Tendon tunneled through the calcaneus for distal fixation
-
-
Achilles allograft:
-
Used for defects greater than 6 centimeters
-
-
Synthetic grafts:
-
Include carbon fiber and polypropylene
-
Avoid donor site morbidity
-
Postoperative Management Protocol
-
Immobilization in above-knee cast or slab with 20 degrees plantar flexion for 2 weeks.
-
Posterior splint in plantar flexion from 2 to 4 weeks.
-
Suture removal at 14 to 18 days.
-
Between 2 and 4 weeks:
-
Allow passive plantar flexion
-
Allow active dorsiflexion
-
-
From 4 to 6 weeks:
-
Begin partial weight bearing
-
Initiate physiotherapy
-
-
From 6 to 8 weeks:
-
Remove heel raise
-
Start passive dorsiflexion stretching
-
-
From 8 to 12 weeks:
-
Progress to full weight bearing with crutch support
-
Continue strengthening exercises
-
Gradual discontinuation of crutches by 12 weeks
-
Complications of Surgical Management
-
Skin necrosis
-
Infection
-
Hematoma formation
-
Wound dehiscence
-
Risk factors include smoking, female gender, steroid use, and open repair techniques
-
-
Chronic ulcer or sinus formation
-
Re-rupture
-
Secondary deformities:
-
Equinus or valgus deformity with overtight repair
-
Dorsiflexion lag with lax repair
-
-
Sural nerve injury, particularly with percutaneous techniques
Leave a Reply