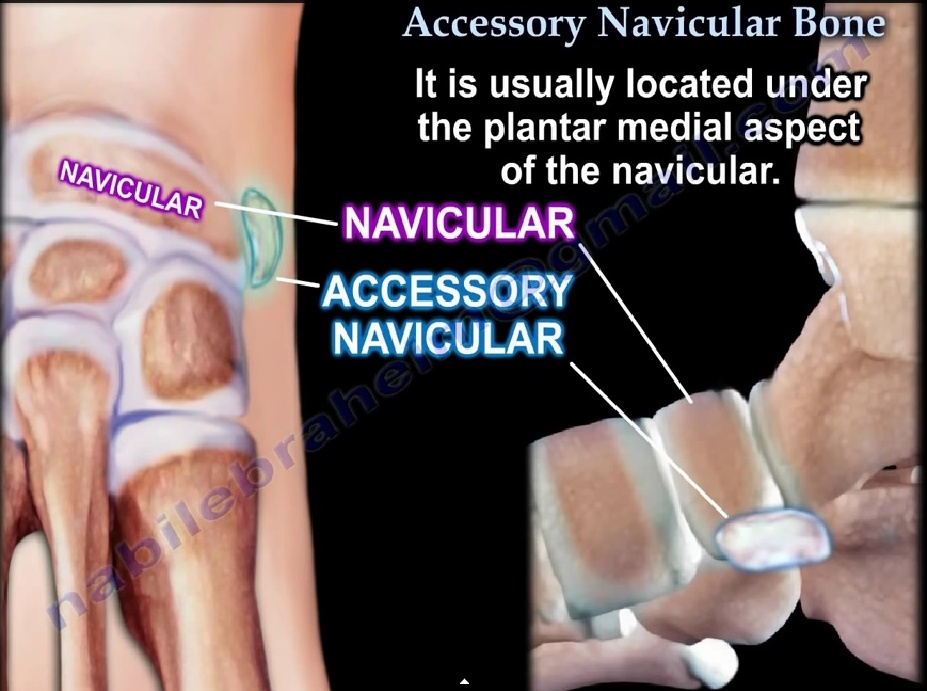
Accesory Navicular
- This anatomic variant consists of an accessory ossicle located at the medial edge of the navicular
- Accessory ossicles are derived from unfused ossification centers.
- 90% bilateral
- It is most commonly symptomatic in the 2nd decade of life and causes medial foot pain
- Symptomatic in <1% of patients.
Classification
- Type I occurs primarily as a round sesamoid within the substances of the distal posterior tibial tendon.
It is rarely associated with symptoms.
Small, 2–3-mm sesamoid bone in the PTT; referred to AS “os tibiale externum”
- Type II is associated with a synchondrosis within the body of the navicular at risk for disruption either from traction injury or shear forces in the region.
Larger ossicle than type I
Secondary ossification center of the navicular bone
Most common variety (50%)
- Type III, also known as a navicular beak or a cornuate navicular occurs with fusion of the accessory navicular bone to the body of the navicular.
Clinical Features:
– Pain may begin after wearing ill-fitting shoes, with weight bearing activities or athletics, or after trauma to the foot.
– Tenderness over the medial aspect of the foot and over the accessory navicular bone.
– Secondary Achilles tendon contracture can occur
– Flatfoot is common and with severe flatfoot, lateral pain may occur secondary to impingement of the calcaneus against the fibula.
X-rays:
– AP, lateral, internal oblique and external oblique
– The accessory ossicle may be best visualized on the internal oblique view(reverse oblique view)
Treatment
• Conservative measures: Shoe-wear modification, including use of a softer, wider shoe, NSAIDS
• Medial arch support for flatfoot.
• A below knee cast may be worn for 3 -6 weeks for persistent symptoms
• Surgery maybe employed for persistent pain not responding to conservative measures
• Kidner’s procedure: Consists of excising the accessory navicular and rerouting the tibialis posterior tendon into a more plantar position.
• Kidner’s operation will not correct sag at the metatarsocuneiform joint.
• Severe flatfoot deformity with lateral impingement symptoms may require concomitant osteotomy of the calcaneus and/or medial column of the foot to improve alignment and decrease mechanical stress of the PTT insertion.
Ref:
- Sella EJ, Lawson JP, Ogden JA. The accessory navicular synchondrosis. Clin Orthop Relat Res 1986;209:280–285
Leave a Reply