Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Introduction
-
Acetabular fractures are among the most complex and serious injuries treated by orthopaedic surgeons.
-
In 1964, Judet and Letournel described a classification system that remains the most widely used method for categorizing acetabular fractures.
-
These fractures most commonly result from high-energy trauma, although they may also occur following low-energy mechanisms in the elderly population.
Epidemiology
-
Incidence is approximately 3 per 100,000 population per year.
-
More common in males than females.
-
Demonstrates a bimodal age distribution:
-
Younger patients: high-energy trauma
-
Elderly patients: low-energy falls
-
Anatomy of the Acetabulum
The acetabulum is composed of 6 principal components:
-
Anterior column
-
Posterior column
-
Anterior wall
-
Posterior wall
-
Acetabular dome (tectum)
-
Medial wall
-
The acetabulum covers approximately 170 degrees of the femoral head.
-
The acetabular dome represents the primary weight-bearing surface.
Mechanism of Injury
-
Younger patients
-
High-velocity trauma
-
Motor vehicle collisions
-
Falls from height
-
Extreme sports injuries
-
-
Elderly patients
-
Low-velocity trauma
-
Fall from standing height
-
Clinical Presentation
-
History of high-energy trauma or fall.
-
Inability to stand or bear weight.
-
Painful and restricted movement of the affected lower limb.
-
Bruising or contusion in the perineal or groin region.
-
Possible neurological deficit, such as foot drop.
-
Frequently associated with other systemic injuries.
Imaging
Radiography
-
Pelvis anteroposterior view.
-
Judet oblique views:
-
Iliac oblique view
-
Obturator oblique view
-
Computed Tomography
-
Computed tomography scan with 3-dimensional reconstruction is essential.
-
Provides:
-
Detailed understanding of fracture morphology
-
Assessment of comminution
-
Identification of marginal impaction
-
Preoperative planning guidance
-
Magnetic Resonance Imaging
-
Mainly indicated in paediatric acetabular fractures.
-
Useful for evaluating labral injury, especially following traumatic posterior hip dislocation.
Classification
Judet–Letournel Classification
Acetabular fractures are classified into elementary and associated fracture patterns.
Elementary Fractures
(Single fracture line resulting in two fragments)
-
Posterior wall
-
Posterior column
-
Anterior wall
-
Anterior column
-
Transverse fracture
Associated Fractures
-
Posterior column with posterior wall fracture
-
Transverse fracture with posterior wall fracture
-
Anterior column with posterior hemi-transverse fracture
-
T-type fracture
-
Both-column fracture
Management
Initial Management
-
Follow Advanced Trauma Life Support principles.
-
Focus on resuscitation and stabilization.
-
Perform focused assessment with sonography for trauma and computed tomography of the abdomen and thorax to identify sources of bleeding.
-
Associated hip dislocation must be reduced urgently.
-
Post-reduction computed tomography scan is mandatory to assess concentric reduction and intra-articular fragments.
Definitive Management
Conservative Management
Indicated for:
-
Stable fractures.
-
Concentric reduction of the hip joint.
-
Fractures not involving the weight-bearing acetabular dome.
Operative Management
Indicated for:
-
Hip joint instability.
-
Incongruent joint reduction.
-
Intra-articular loose bodies, including bone or soft-tissue interposition.
Surgical Fixation Options
-
Open reduction and internal fixation with plates and screws.
-
Percutaneous screw fixation:
-
Antegrade
-
Retrograde
-
-
Total hip arthroplasty in selected cases, particularly in elderly patients with comminution or pre-existing arthritis.
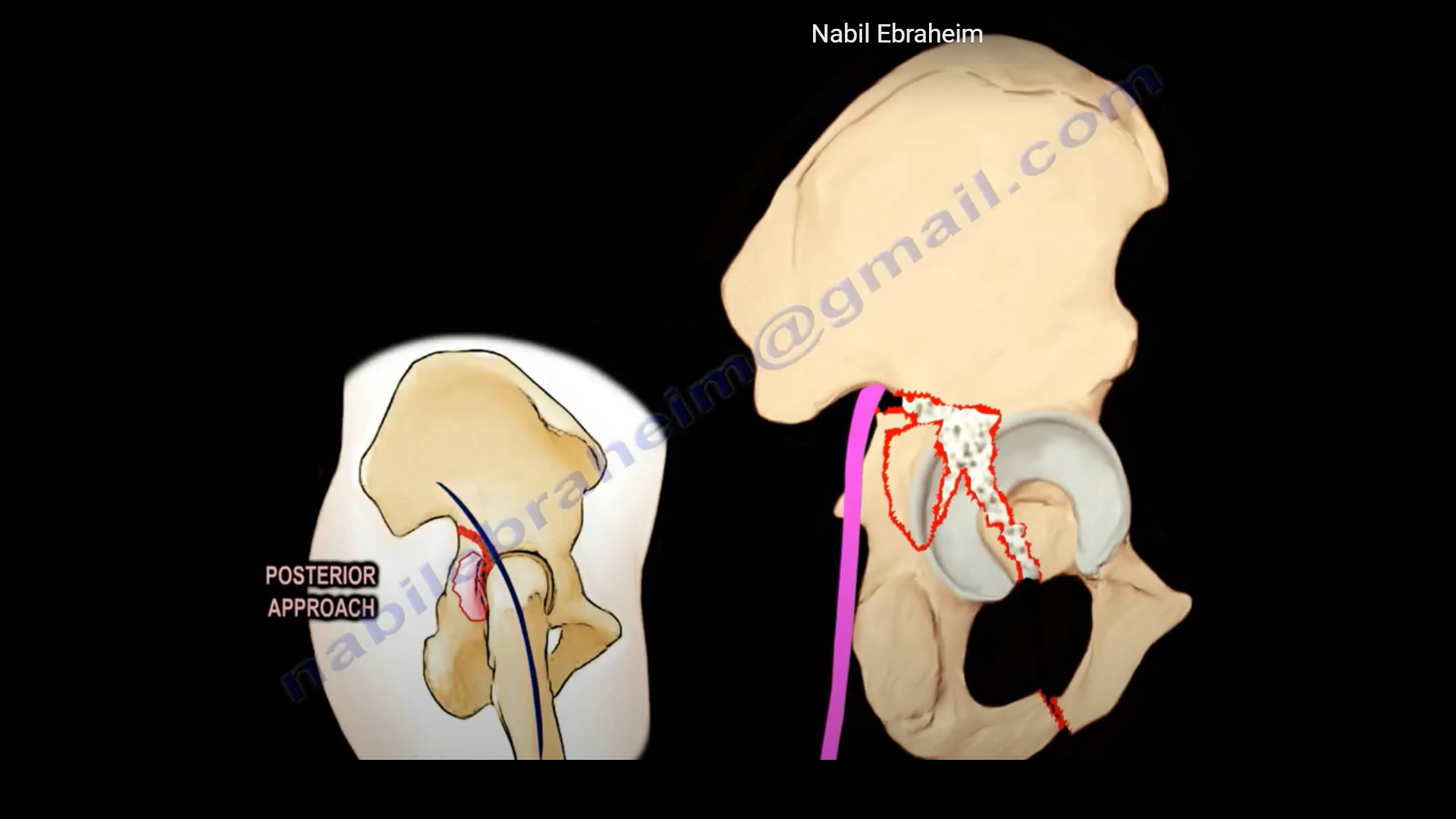
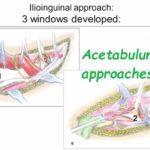
Surgical Approaches
-
Posterior approach (Kocher–Langenbeck approach).
-
Ilioinguinal approach.
-
Modified Stoppa approach.
-
Combined anterior and posterior approaches.
-
Iliofemoral approach.
-
Extended iliofemoral approach.
-
Triradiate approach.
Complications
-
Surgical site infection.
-
Deep vein thrombosis.
-
Persistent hip subluxation or instability.
-
Avascular necrosis of the femoral head.
-
Iatrogenic nerve injury.
-
Heterotopic ossification.
-
Post-traumatic osteoarthritis.
Summary
-
Acetabular fractures are complex injuries requiring meticulous assessment and management.
-
Judet–Letournel classification remains the cornerstone for fracture description and surgical planning.
-
Computed tomography is essential for accurate fracture characterization.
-
Treatment decisions depend on fracture stability, joint congruity, and patient factors.
-
Anatomical reduction and stable fixation are critical to achieving optimal long-term outcomes.


Leave a Reply