Courtesy: Prof Nabile Ebraheim, University of Toledo, Ohio, USA
Anatomical & surgical consideration of Pectoralis Major
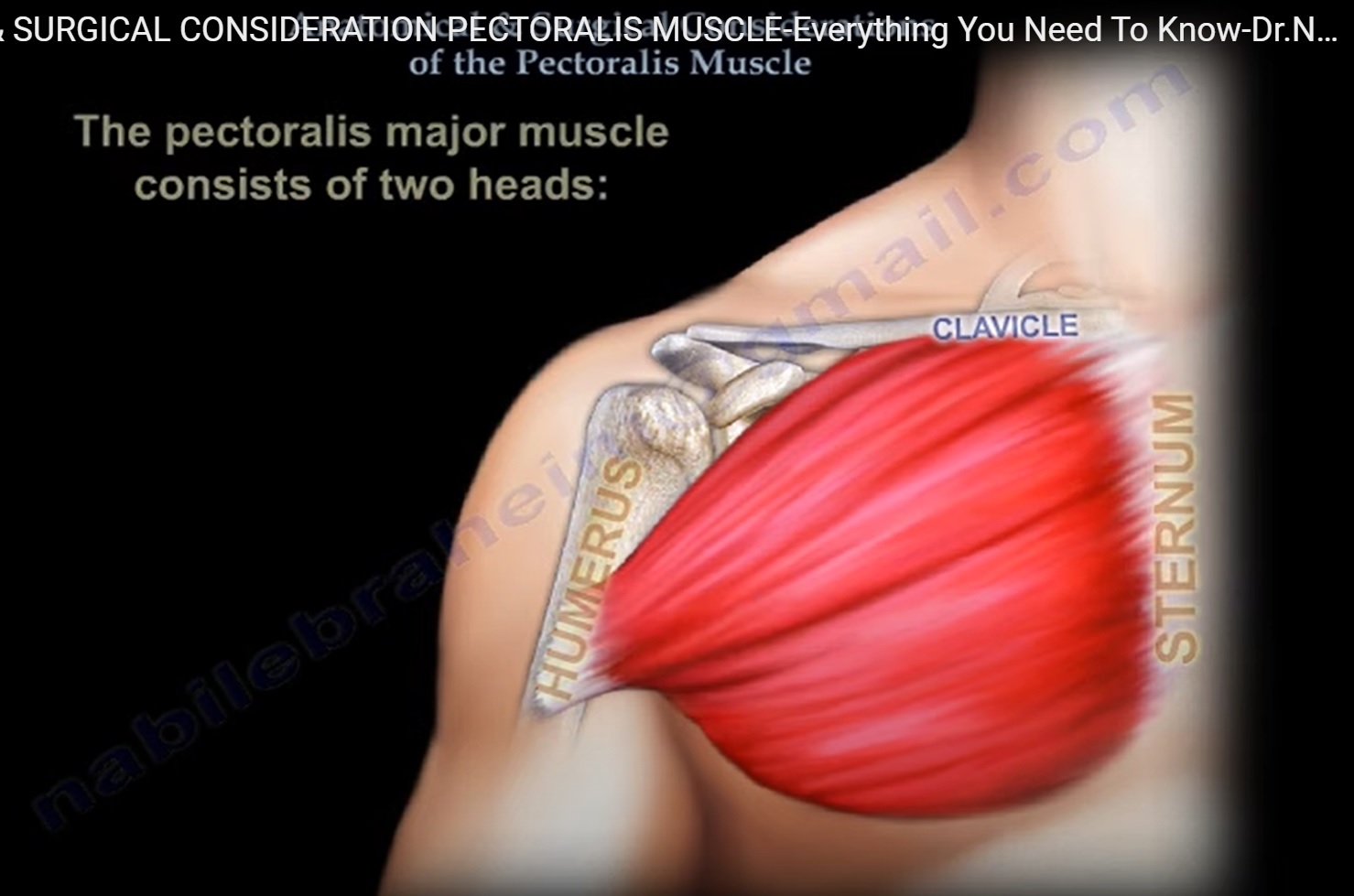
- Pectoralis major extends from Sternum to humerus
- Consists of 2 heads- clavicular head from clavicle to upper humerus
- Sternocostal head – from sternum+first rib Through sixth rib to upper humerus
- Inserted into lateral lip of bicipital groove
- Innervation- medial & lateral pectoral nerve
- Action: Adduction + internal rotation of arm
– Tear occurs in young weight lifters
Symptoms- pain around shoulder, loop feeling on bench press, discoloration + burning sensation over pectoralis major+ axilla, lose of contour of axillary fold, palpable defect
Investigation: MRI to differentiate between complete & partial tear & to locate the tear.
Treatment: reinsertion of tendon into shaft of humerus lateral to biceps groove
Chronic case: tendon graft
POLAND SYNDROME:
- Unilateral chest wall hypoplasia due to the absence of sternocostal head of Pectoralis major
- absence of metacarpals+phalanges
- hypoplasia of hand n forearm
- syndactyly
Pectoralis minor:
- Origin: surface of superior margin of 3,4 n 5 ribs
- Insertion:medial border of coracoid process of scapula
- Innervation: medial pectoral nerve
- Action: stabilizes scapula by drawing scapula inferiorly and anteriorly
Leave a Reply