Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
- Shoulder dislocation is dislocation of the head of the humerus from the glenoid, which is a part of the scapula.
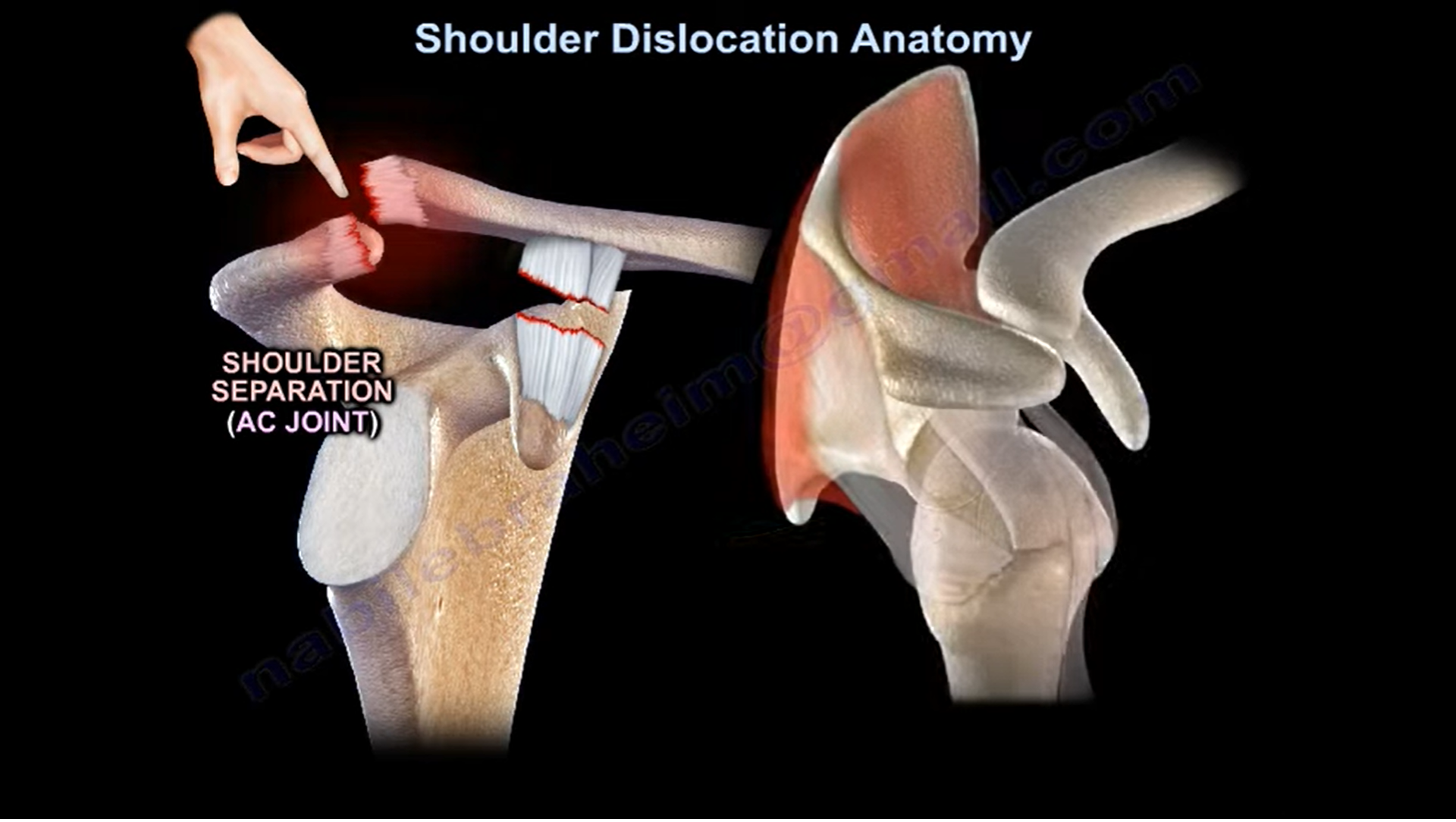
- The acromioclavicular joint is called the ac joint. When it is injured they call it shoulder separation.
- Shoulder dislocation is different from shoulder separation.
- The most common associated lesions with dislocation of the shoulder are Bankart lesion, Hill- Sachs lesion, Rotator cuff tear in the elderly, Axillary nerve injury and the greater tuberosity or lesser tuberosity fractures.
- The shoulder joint is the joint between the head of the humerus and the glenoid. The labrum is attached to the glenoid.
- The labrum reinforces the glenoid cavity and acts like a bumper within the joint capsule of the shoulder joint. It deepens the socket by about 50%.
- During shoulder dislocation there will be injury to the labrum and it is called a Bankart lesion.
- Bankart lesion is associated with a high recurrence rate of dislocation especially in young patients. Bankart lesions are present in about 80 to 90 percent of patients with TUBS.
- TUBS is a traumatic unilateral bankart lesion requiring surgery. Bankart lesions can be fibrous or bony due to avulsion of the anterior labrum and anterior band of the inferior glenohumeral ligament from the anterior inferior glenoid.
- Bony Bankart will be present in about 50% of patients with recurrent dislocation. Bony deficiency of the glenoid of 20 to25% or less will make the shoulder very unstable and arthroscopic surgery alone with soft tissue repair is not sufficient.
- Deficiency of the glenoid 20 to 25% or less will probably need a bony augmentation procedure for the glenoid.
- The best study to know the exact or accurate deficiency of the glenoid is a CT scan of the glenoid with 3D reconstruction. With failure rate up to two-thirds of the patients, you need a bony augmentation procedure such as the Latarjet procedure, when you transfer the coracoid to the glenoid. You may also use an iliac crest bone graft.
- Latarjet for glenoid bone loss more than 20 to 25% especially in inverted bare deformity of the glenoid.
- Cuff tears occur more in the elderly with dislocation of the shoulder.
- About 30 percent of patients are more than 40 years old and 80 percent of patients are more than 60 years old.
- If the patient is unable to lift the arm after reduction of shoulder dislocation and the patient is young think about Axillary nerve palsy and if the patient is old think about Rotator cuff tear.
- As the head of the humerus impacts against the anterior inferior edge of the glenoid, a lesion is created in the posterior superior aspect of the humeral head called Hill-Sachs lesion. It is present in about 80 percent of acute traumatic dislocation and in about 25 percent of traumatic subluxation.
- Remplissage procedure is used for Hill-Sachs lesions if the defect is large (more than 25 percent). The posterior capsule and the infraspinatus tendon are sutured into the Hill – Sachs defect.
- In posterior shoulder dislocation, the lesser tuberosity can be fractured. If you have posterior dislocation less than six months and the reverse Hill – Sachs lesion less than forty percent of the humeral head, you will do open reduction and subscapularis transfer (Mclaughlin procedure) or lesser tuberosity attached to the subscapularis transferred to the defect.
- So how about the HAGL lesion. It is humeral avulsion of the inferior glenohumeral ligament. It is seen more in violent sports injuries. It is uncommon and it is unrecognised and it can cause recurrent shoulder instability. It is associated with a higher recurrence rate if not recognized and repaired and the mri will show the inferior pouch irregularity.
- How about the anterior inferior glenohumeral ligament- it is an important ligament. It is an injury that will cause anterior translation of the humeral head at 90 degrees of abduction and external rotation at the apprehension position.
- The posterior inferior glenojhumeral ligament this injury will cause posterior translation at 90 degree flexion and internal rotation. In general anterior labral tear injury is seen in the axial view on an mri. The image is enhanced by a dye and the anterior instability is diagnosed by apprehension test. The biceps groove is anteriorly. Posterior labral injury will cause posterior instability and causes more pain than instability. The posterior labral tear is seen in the axial view on the mri. You can diagnose this injury clinically by the Jerk test or the Kim test.
- Why are posterior shoulder dislocations most commonly in seizures and electric shock?
- Because the shoulder internal rotators (the subscapularis, the latissimus dorsi and the pectoralis major) are stronger than the external rotators. Watch out for normal variants of the labrum that looks like an injury but not an injury. Normal variance of the labrum are the sublabral foramen or the Buford complex.
- Do not repair them because patients can lose motion, especially external rotation.
Leave a Reply