Courtesy: Prof Abhijeet Wahegaonkar, Sancehti Hospital, Pune, India
Introduction
• Robert Kienbock- radiologist. Described xray changes associated with lunatomalacia.
• an isolated disorder of the carpal lunate arising out of vascular compromise
• multifactorial pathogenesis- influenced by genetic, anatomic, mechanical and metabolic factors.
Historical perspectives
- first described by Peste in 1843 who noted a collapsed lunate in cadaver dissection
- Robert Kienbock- radiologist. Described Xray changes associated with
Kienböck’s disease
Etiology
- etiology is still undefined so various factors have been proposed
- aberrant blood supply to lunate: problems with arteries[single dominant nutrient arterial supply for lunate (20%patients)
- poorly organized intraosseous circulation —“i”pattern of anastomosis
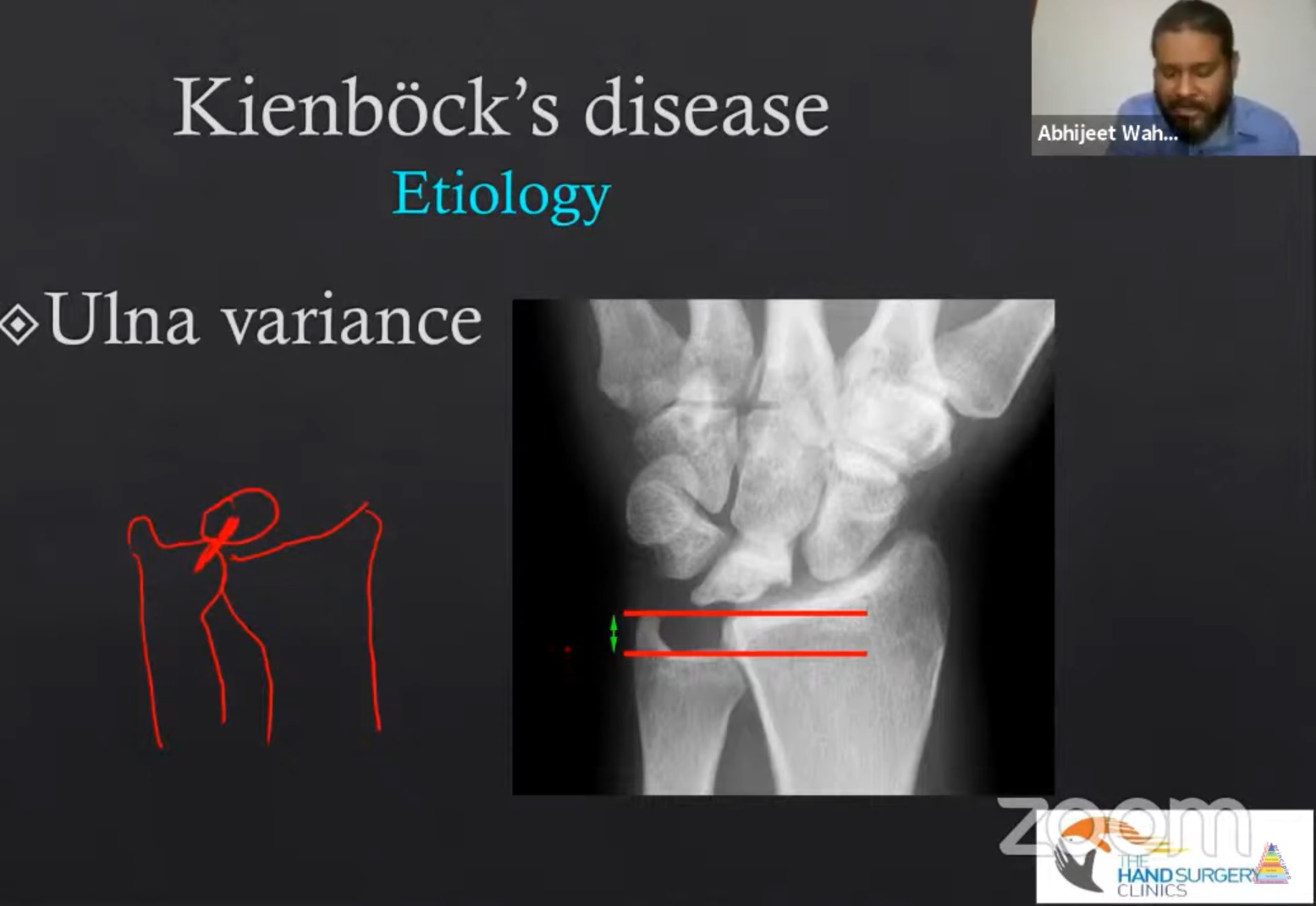
- ulnar variance (radioulnar index) = distance between distal point of ulna on radial side and the distal point of radius on ulnar side. Normal is ±2, -2 means ulna is 2 mm shorter than radius.
- lunate geometry
- mechanical injury
Diagnosis:
- symptoms can vary depending upon the stage at initial presentation.
- pain localised to the radiolunate facet pain is classically insidious in onset
- pain and stiffness in the dominant wrist
- decreased grip strength
hyperextension injury
Radiographs
X-ray imaging during stage 1 of the disease will show an apparently normal lunate bone, later sclerosis, fracture, fragmentation and collapse are seen.
Bone scan
o nonspecific
o does not rule out early AVN
Trispiral tomography
more accurate staging than x-ray alone
• does not rule out early AVN
CT scan
• provides useful detail of fracture fragments
Mri
• sensitive, specific
- magnetic resonance imaging can help to assess the blood supply to the lunate.
- The gadolinium-infused mri has been used to find the vascular patterns
abnormal signal in 50% of lunate
Staging
- Lichtman modification of Stähl’s classification
• stage 1-4
• modified by Amadio - stage 1- no visible changes on radiograph; changes seen on mri.
- stage 2- sclerosis of lunate
- stage 3a- fragmentation of lunate
- stage 3b- fixed rotation of scaphoid
- stage 4- degeneration of adjacent intercarpal joints
Treatment
- based on the stage at presentation
- unload the lunate
- revascularise the lunate
- treat carpal instability and collapse with salvage procedure
Stage 1
• conservative treatment with 3 months immobilisation is typically recommended for stage 1 disease
- the patient should continue to be monitored and if symptoms or radiographs progress consider surgical management.
Stage II or III with negative ulnar variance
- goal in this stage is generally centered towards unloading of lunate is an attempt to reduce
intracarpal stress and allow revascularization.
Joint levelling procedures-
• radial shortening osteotomies
• ulnar lengthening procedures
Radial osteotomy is preferred over ulnar due to less complication
Stage II and 3a ulnar neutral or positive variance
- revascularisation
- osteotomies
- core decompression
Stage 3b
o goal in this stage
o stabilization of carpus
o prevent further collapse
Decrease the load across radiolunate joint
- proximal row carpectomy
• scaphotrapeziotrapezoid arthrodesis
• scaphocapitate arthrodesis
• grafting ,arthroplasty and interposition
Stage iv
• salvage procedures performed.
• wrist arthrodesis
• wrist arthroplasty
• wrist denervation.
Summary
- Kienbock disease is defined by AVN of lunate, with a predictable pattern of lunate collapse .carpal changes, and degeneration resulting from an apparent combination of vascular, anatomical and traumatic insults
Leave a Reply