Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
ANATOMY OF ILIOPSOAS MUSCLE
INTRODUCTION:
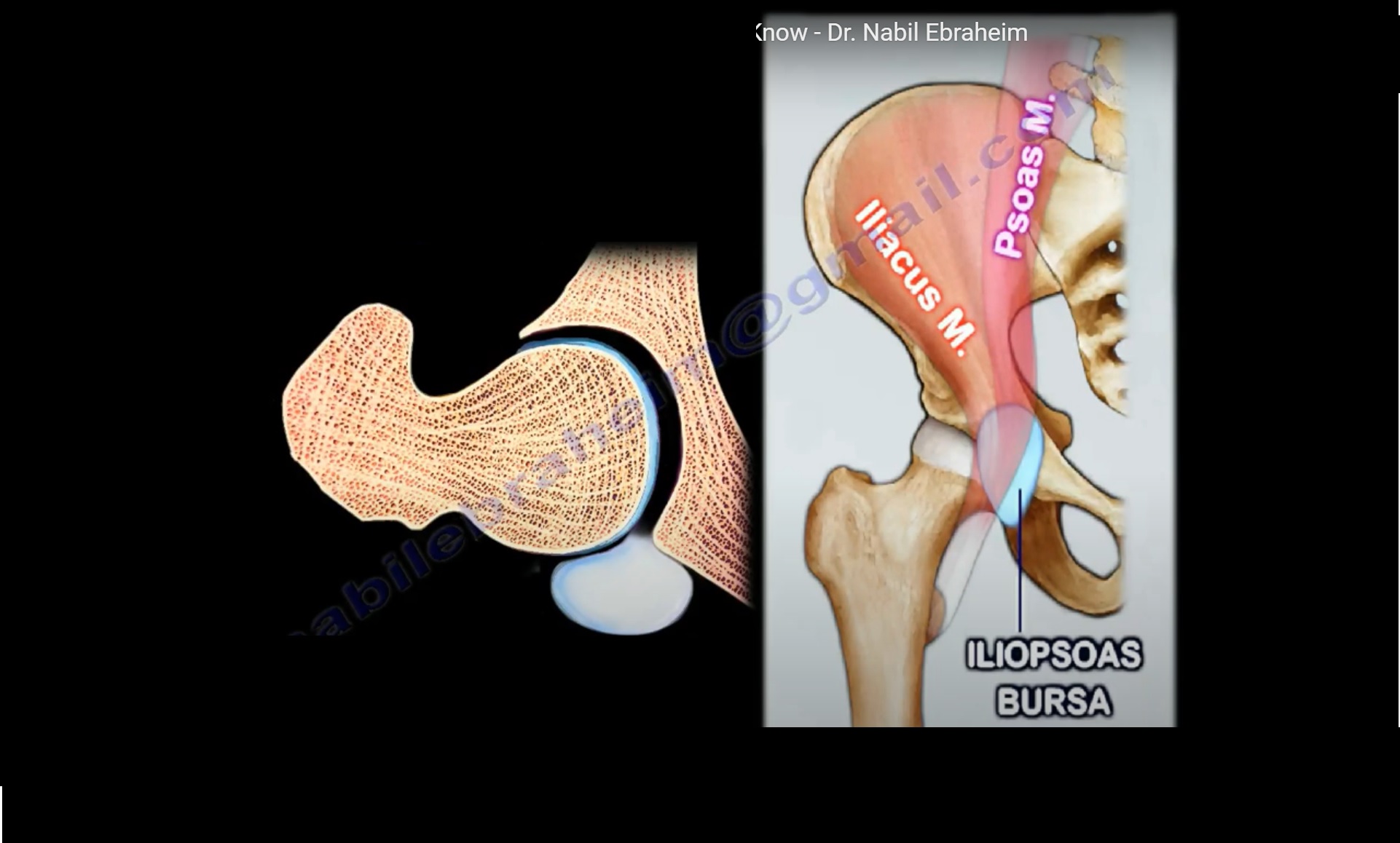
IT INCLUDES 3 MUSCLES : PSOAS MAJOR,PSOAS MINOR(if present),ILIACUS.
PSOAS MAJOR
ORIGIN : It arises from the transverse processes and lateral aspect of vertebral bodies T12 – L5.
COURSE :Runs downwards across the pelvic brim and then passes deep to the ilioinguinal ligament and then forms a tendon past hip joint capsule.
INSERTION : Inserts into lesser trochanter of femur.
NERVE SUPPLY: L1,L2,L3 OF Lumbar plexus.
FUNCTION : Flexion of hip.
ILIACUS
ORIGIN :
a)from iliac fossa on the inner side of ilium.
b)anterior inferior iliac spine.
INSERTION : Lesser trochanter of femur.
NERVE SUPPLY : Femoral nerve.
FUNCTION : Flexion of hip joint.
ASSESSMENT OF ILIOPSOAS MUSCLES
Ask the patient to lift the knee straight up from the examination table,examiner then applies downward pressure onto the knee inorder to assess the hip flexion strength.
ILIOPSOAS COMPARTMENT SYNDROME
The extraperitoneal space in which these muscles are present is known as iliopsoas compartment.
CAUSES :
1)Haemorrhage.
2)Severe trauma.
3)Anti-coagulation therapy.
4)Haemophilias or other blood diseases.
CLINICAL PRESENTATION :
1)Flexion attitude.
2)Pain with passive extension.
3)Tenderness along the ilioinguinal ligament.
4)Parasthesia around the medial side of the knee.
DIAGNOSIS : MRI or CT.
TREATMENT :
1)Conservative management with correction of coagulation defect if present.
2)Surgical intervention is rarely needed
ILIOPSOAS ABSCESS.
- The abscess in the iliopsoas compartment is known as iliopsoas abscess.
- The primary abscess is caused by hematogenous spread of infection.
- The secondary abscess ,the infection spreads from another area to psoas muscle.Eg :the infection may travel from the spine to the muscles when it is infected by Tuberculosis(Pott’s disease).
- It can also spread from the adjacent structures like sacro-iliac joint,kidneys or bowels.
Clinical features: Patient lies supine with hip flexed and refuses to move resisting any attempt for examination.Pain in abdomen,flank,groin and low back ache.Low grade fever.Limited and painful range of motion.
DIAGNOSIS :
1)Psoas sign-the patient is made to lie down on the side and then the hip is extended to see if there is pain in the iliopsoas region.
2)MRI.
SNAPPING HIP SYNDROME
It is a condition involving the iliopsoas bursa(bursa between iliopsoas tendon and hip joint)in which an audible snap or click of iliopsoas tendon occurs over the iliopectineal eminence.
This audible click or snap sensation usually occurs with hip movement which may or may not be painful.
SUBTROCHANTERIC FRACTURE
In subtrochanteric fracture, iliopsoas muscle flexes proximal fragment of femur which complicates the reduction of fracture.
OTHER IMPORTANT CLINICAL CONDITIONS
1)Iliac vessels are 1 cm away from the iliopsoas at the level of pelvic brim and 3 cm from the iliopsoas at the level of lesser trochanter. Tenotomy of iliopsoas during the anteromedial approach for reduction of congenitally dislocated hip causes injury to medial circumflex femoral artery.
2)In total hip replacement,leaving the anterior rim of the acetabular component above the acetabulum may result in impingement of iliopsoas tendon.Patient presents with groin pain or pain with passive extension.Evaluate the patient with an X-RAY and CT scan and give the patient an injection into the tendon sheath and revision surgery may be necessary
Leave a Reply