Courtesy: Rishi Dhir, Consultant Orthopaedic Surgeon, Princess Alexandria Hospital and CEO, Lets Talk Dr
To crack any bone tumor and its prognosis we need to focus on mainly 5 points
- First we look for which bone is involved for Example femur, tibia etc and later we look for the location of the particular bone involved such as physis, metaphysis, epiphysis, diaphysis etc. Along with these we classify it as whether concentric or eccentric
- Secondly we look for the outline of the lesion. For example it may be a well demarcated like a geographic lesion with a narrow zone of transition. Such a lesion is usually less aggressive, whereas if the lesion has blurry margins or looks polydefined with wide zone of transition it is more a type of aggressive tumor
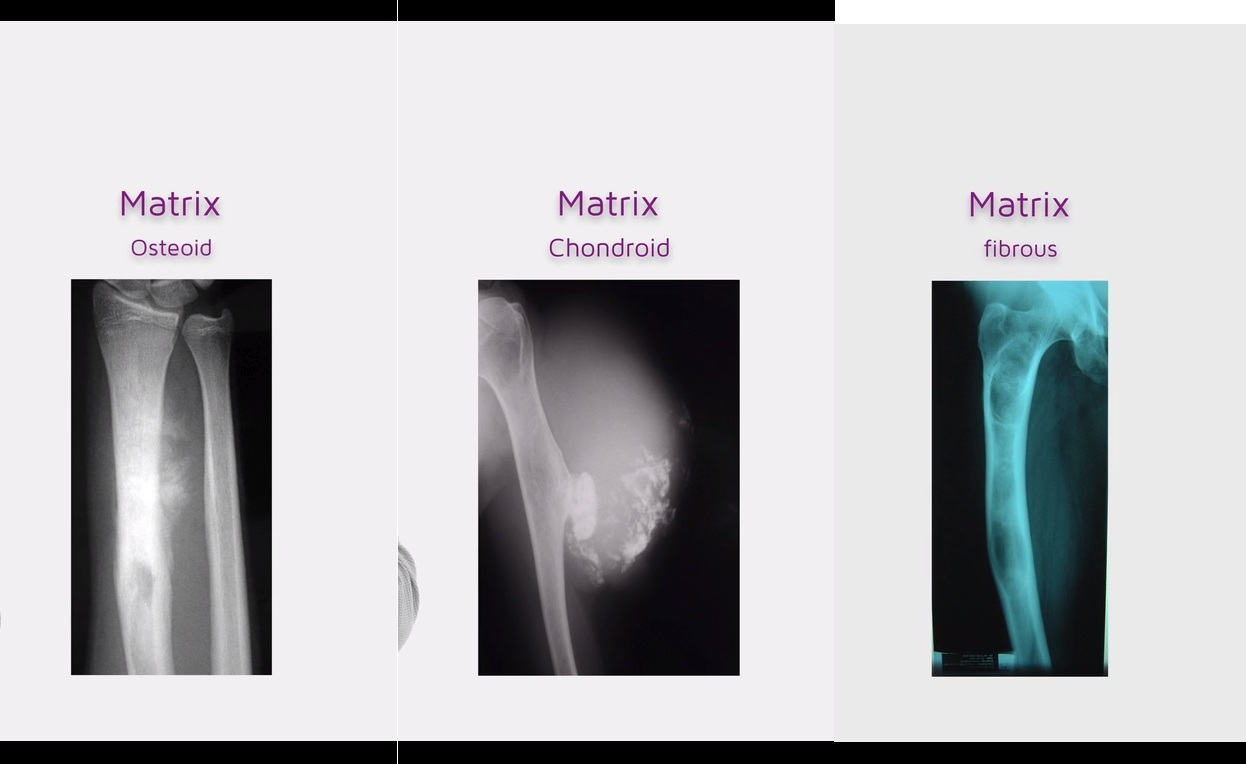
Next we look for the matrix of the lesion. It may be osteoid or chondroid or fibrous/ground glass - We also need to look for the periosteal bone reactions.. Lesions may not remain inside the bone matrix and may cause several reactions at the periosteum due to pressure effects such as Codmans triangle or sunray spiculations
- Finally we look for the surrounding soft tissue reaction such as edema, rise of temperature, color changes etc
Before starting treatment for any tumor we need to do TRIPLE ASSESMENT for staging and assessment of lesion which includes
1-clinical assessment 2- radiological assessment 3- tissue diagnosis
In the Clinical assessment we need to get a detailed history of the patient which includes risk factors, constitutional symptoms, family history, any primary lesions, red flag sign(night pain etc).We also need to do a thorough examination of the swelling, and whole body to look for any palpable lymph nodes, chest and abdomen must be thoroughly examined to rule out any primary malignancy or metastasis
Coming to the Radiological assessment we need to have a plain radiograph of whole limb to know about the extent and area of lesion along with a MRI to rule out focal skip lesions in the surrounding areas or soft tissues. CT Chest/abdomen /pelvis also must be taken as routine investigation to rule out distant lesions
Finally the TISSUE DIAGNOSIS. For extracting tissue from the lesion we either opt for a jamshidi needle, Or else we chose for a trucut biopsy from the site
Principles of taking biopsy includes it should be performed at same centre and same surgeon. Must be Unicompartmental and the surgeon must attain Hemostasis. The Drains must be excised in same tract and Biopsy peripheral site should also be taken for defining the extent of lesion
A tumor usually have 2 zones. A necrotic centre and a zone of reaction
Dealing with the surgical resection we have 4 types of resection which include
- Intralesional
- Marginal
- Wide
- Radical
Staging system of the tumor commonly used is Enneking system which is based on Grade (G), local extent (T) and metastasis (M)
Grade
G1-low grade –
G2- high grade
Local extent
T1- intracompartmental (A)
T2-extracompartmental (B)
Metastais
M0-no mets
M1-mets present
Stage 1A-low grade, intracompartmental, no mets
Stage 1B-low grade, extracompartmental, no mets
Stage 2A-high grade, intracompartmental, no mets
Stage 2B- high grade, extracompartmental, no mets
Stage 3- any G, any T, mets +
The primary Goals of treatment includes Save life, Save limb if not possible at least Preserve function with limb reconstruction procedure or salvage surgery
- Other than surgical resection we also have chemotherapy, radiotherapy as other treatment modalities. But the choosing of treatment Depends on type of tumor.
- For example in a diagnosed case of osteosarcoma we need neoadjuvant therapy +surgery +adjuvant therapy. Any procedure Requires 90 percent necrosis rate.
- But in case of Chondrosarcoma- surgery is the primary option because it Doesn’t respond well to chemo/ radiotherapy like osteosarcoma
Leave a Reply