Courtesy: Dan Zlotolow, Shirner’s hospital for Children, USA
ARTHROGRYPOSIS MULTIPLEX CONGENITA
Spectrum of disorders (symptom complex)
• Diminished fetal movements
• Congenital joint stiffness
• Varying degrees of muscle weakness
INTRODUCTION
• Greek word means “bent joint“
• Condition first described in 1841
• The term ‘Arthrogryposis Multiplex Congenita’ coined by WG Stern in 1923
Definition
• Arthrogryposis is used to denote nonprogressive conditions characterized by multiple joint contractures found at birth & It involves contractures of at least two joints in two different body regions.
• Incidence:
1 in 3000 live births
True amyoplasia – 1 in 10,000 live births
TYPES
• Classic arthrogryposis called amyoplasia (not inherited)
• Distal arthrogryposis ( 6-10 subtypes)-Hall’s and Bamshad classification
Hall’s Classification of AMC
1. Primarily Limb Involvement
2. Limb involvement+ Visceral anomalies
3. Limb + CNS involvement
CAUSE
• Genetic ( Distal arthrogryposis)
• Virus (coxsackie virus)- post viral autoimmune attack on acetyl choline receptors
Vascular interruptions Divided into Intrinsic factors and Extrinsic factors
Intrinsic Factors
• Intrauterine Vascular Compromise
• Severe bleeding
• Failed termination
• Monozygotic twins
• Amniotic Bands
• Maternal Considerations
• Multiple Sclerosis
• Diabetes Mellitus
• Myasthenia Gravis
• Maternal Infection
• Drug Exposure
Extrinsic Factors
• mechanical obstruction
• Fetal crowding: multiple births
• Oligohydramnios
• Uterine Fibroids
• Trauma
Genetics of arthrogryposis
• Sporadic mutation (amyoplasia)
• Single-gene mutations
• Chromosomal disorders (e.g. trisomy 18)
• They leads to absence of active fetal movements (akinesia)-(normally fetal movements starts in the eighth week of fetal life).
• Fetal akinesia lasting over 3 weeks may be sufficient to develop AMC.
• Consequently fetal akinesia leads to fibrosis and contractures of the affected joints.
Clinical features
• Amyoplasia or classic arthrogryposis:
• A – absence, myo – muscle, plasia – development(non-development of muscles).
• It is a sporadic multiple contractures syndrome.
• The central nervous system function is normal
• The muscle tissue is often replaced with fatty and fibrous tissues
Upper limb
• Shoulder: Adducted and internally rotated.
• Deltoid muscle function is deficient.
• Extended Elbow
• Palmar flexion contracture with ulnar deviation of wrist
• Intrinsic Plus Hand
• Thumb is usually adducted.
Lower limb
• Hip: Mostly flexion, abduction, and external rotation contractures(FABER)
• Unilateral or bilateral hip dislocation/subluxation can be observed
• Knee: flexed / extended
• Feet: CTEV/CVT
Spine
• Abnormal curvatures in approximately 28% to 67% of patients
• C- shaped scoliosis
• The curves often rapidly progress
Extra skeletal manifestations
• Facial skeleton –
• Hypoplasia of the mandible (micrognathia).
• Contracture and limited function of temporo-mandibular joints.
• Normal intelligence
• Hemangioma on the forehead.
• Abdominal wall abnormalities(inguinal hernia or gastroschisis)
• Reproductive abnormalities.
Distal Arthrogryposis
• Contractures limited mainly to the distal portions of the limbs, i.e. to wrists, hands, ankles, and joints of the foot.
• In hand- ulnar deviation of fingers + flexion deformities of IP joints
• Hand is often called ‘cup like palm’
• In Foot- metatarsus adductus+CVT / club foot
Other conditions that mimic Arthrogryposis(can be inherited)
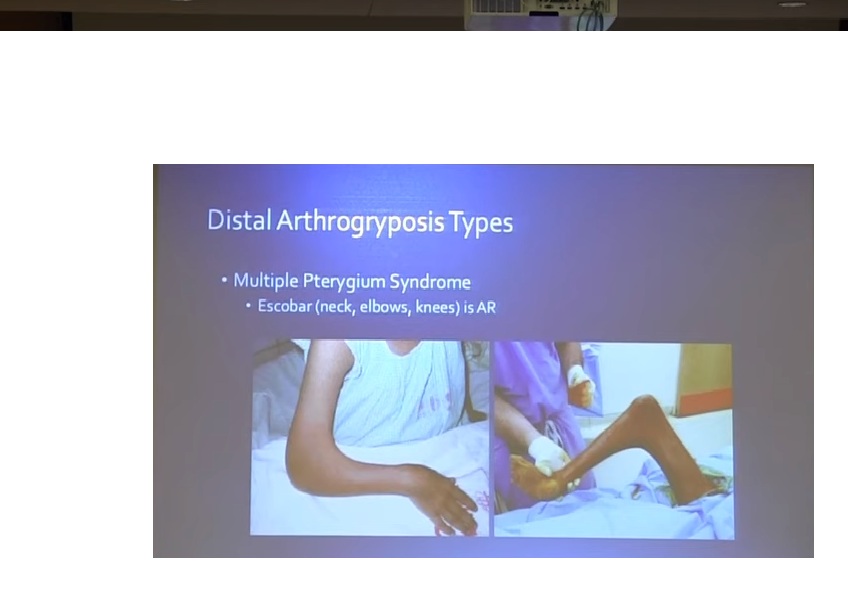
• Papas syndrome (Pterygium syndromes )
• Escobar’s syndrome (multiple pterygium syndrome)
• Larsen syndrome
• Bruck syndrome
Classification
Upper Limb
• Type 1 – Shoulder- Adduction+ IR
Elbow- Extended+ Pronated Forearm
Wrist- Flexion +Ulnar Deviation
• Type 2 – Shoulder- Adduction+ IR
Elbow- Flexed+ Pronated Forearm
Wrist- Flexion +Ulnar Deviation
Lower limb
• Type 3 – Hip – Flexion + Adduction with dislocation
Knee – Extended
Foot – Equinovarus
• Type 4 – Knee – Flexion
Foot – Equinovarus
• Type 5 – Hip – Flexion + Abduction
Knee – Flexion
Foot – Equinovarus
• Type 6 – Hip – Flexion
Knee – Extension +Valgus
Foot – Equinus
• Type 7 –Foot – Equinus
• Type 8 –Foot – Equinovarus Foot + Weak Intrinsic Muscles Of Foot
Treatment
• These children are quite intelligent and sensitive to pain
• The principal goal is optimization of quality of life: this includes
unassisted activities of daily living
independent ambulation
Independent living
social participation capacity
TRIAD OF TREATMENT TOOLS:
• I) Rehabilitation including physiotherapy, manipulation of contractures, and later social and occupational rehabilitation.
• II) Orthotic management, for maintenance or correction of deformities.
• III) Surgical techniques for correction of musculoskeletal deformities
Rehablitation and Physiotherapy
• Gentle stretching and ROM exercises
• Passive stretching exercise followed by serial splinting.
• Major Goals
• Plantigrade standing and walking
• Restoring upper limb function to carry out daily living activities
Surgical Management
• Do surgeries to get functional improvement as much as possible in as few surgeries as possible.
• Preferably Finishing By Age Of 6 Years.
• Knee And Hip Surgery – Around 6 To 9 Months
• Foot Surgery – At 6mo to 1 yr of age (before walking)
Upper Extremity
Shoulder:
• Internal rotation rarely causes a problem
• If causing subcapital derotation osteotomy of humerus could be performed.
Elbow Deformities:
• Early splinting & Serial casting.
• Flexion Contractures – surgery not indicated
• Extension Contractures :
• Posterior capsulotomy and triceps tendon lengthening
• Triceps to biceps transfer most common
Steindler flexorplasty- flexor-pronator mass origin transferred proximally to restore elbow flexion
Wrist Deformities:
• Volar flexion and ulnar deviation
• Release of Volar wrist capsule
• Flexor Carpi Ulnaris tendon transfer to Extensor Carpi Radialis Brevis
• Distal radius Osteotomy
• Arthrodesis -In slight palmar flexion
Thumb-in-Palm Deformity:
• Z-plasty: Release Of Adductor Pollicis
• First Metacarpal Osteotomy
• First Metacarpophalangeal Joint Arthrodesis
Spine
• Spinal deformities develop in 30-62% of arthrogryposis patients.
• In moderate deformities, rehabilitation measures are used
• The corrective braces can be used in curvatures of up to 30° of Cobb’s angle
• Surgery: If Cobb’s angle > 40°
• Spinal fusion with instrumentation
• Combined approach (ant/post)
• Treated same way as idopathic scoliosis
Hip deformities
• Hip flexion Contractures are present in nearly 90% of Arthrogryposis children
• Studies to date have not found pain to be a problem with these hips
• Operative procedures have potential to worsen function if they produce significant contractures
• Contracture up to 30°:
• Treatment may be limited to manipulations and orthotic management.
• Flexion contractures over 30-45° :
• Usually require surgical correction as they impair mobilization and result in increased compensatory hyperlordosis of the lumbar spine.
• Release of contracted soft tissues (including the rectus femoris and sartorius, the iliopsoas muscle, and the hip joint capsule)
• In the older child, proximal femoral extension osteotomy.
• Moderate abduction and external rotation hip contractures
Usually do not require surgical treatment as they improve stability during ambulation
Hip Dislocation:
• Unilateral dislocation:
• Bracing, traction, casting – rarely helpful alone.
• Open reduction (6mo-1yr)- Definite for ambulatory patient.
if not –pelvic obliquity and scoliosis
• Medial incision: (if less than 6 months old)
• Anterior incision:(if more than 6 months old)
Bilateral Hip Dislocation:
• can leave it dislocated
• Non-operative: functional ambulation without pain
• Operative: improved quality and efficiency
• Spica cast/ pavlik harness for 6 weeks.
• Supple hip that is dislocated is preferred to a stiff reduced hip.
Knee deformities
• Flexion Contractures (~50%)
• Mild: <15°-20°, Stretching and physiotherapy.
• 20 ° – 40 °- Hamstring lengthening
• Post-op splinting
• Moderate: 40 ° – 50 °- Z-plasty in popliteal fossa
• Post-op serial cast changes
• Severe; 60° – 80°
• Distal femoral extension Osteotomies.
• Extension Contractures:
• Percutaneous release of quadriceps tendon
• V-Y plasty of quadriceps tendon
• Respond better to physical therapy and splinting
Foot and Ankle Deformities
• Club feet:
• Manipulation and serial casting (but generally resistant)
• Surgical treatment at 6mo to 1 yr of age (before walking)
• Aggressive soft tissue releases.
• Long term bracing, night bracing, ankle-foot orthosis
• recurrence of up to 73% but more favored
• talectomy remains an option
• Relapsed foot:
• Talectomy- may cause Tibio calcaneal incongruity & loss of medial column
• Leads to Progressive mid foot adduction, if calcaneo cuboid joint not fused.
• Subtalar arthrodesis
• Triple arthrodesis
Leave a Reply