Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
Tarsal tunnel syndrome
- It is a compression neuropathy of tibial nerve within the tarsal tunnel.
- It is the most common compression neuropathy of ankle and foot.
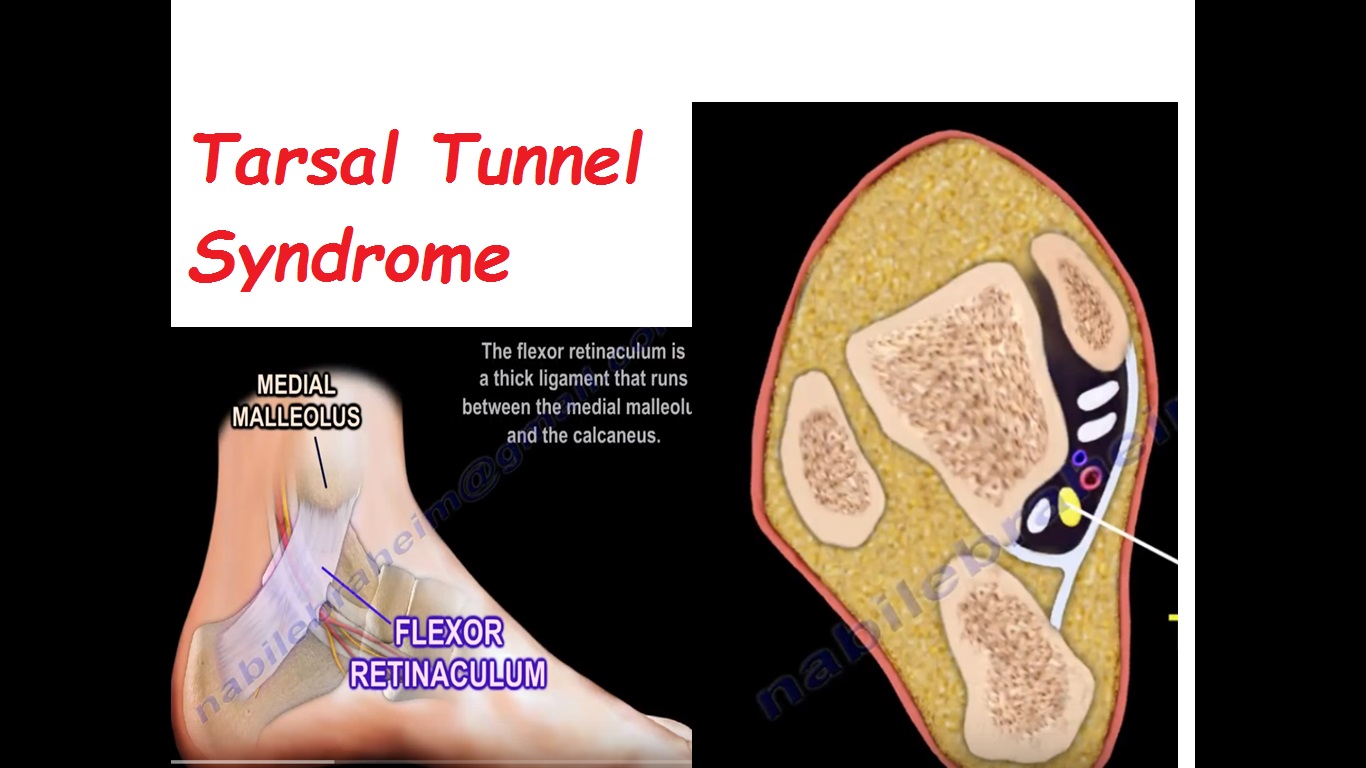
- Tarsal tunnel is a fibro-osseous tunnel posterior and inferior to medial malleolus. The tunnel is covered by flexor retinaculum which is a thick ligament that runs between medial malleolus and calcaneum
Contents of Tarsal tunnel
- Tibialis posterior
- Flexor digitorum longus
- Posterior tibial artery
- Tibial nerve
- Flexor hallucis longus
Causes of Tarsal tunnel syndrome.
- Space occupying lessons – lipomas or ganglion
- Varicose veins
- Muscle anomalies
- Tenosynovitis
- Rheumatoid arthritis
- Diabetes
- Malaligned foot
- History of trauma
Symptoms
- Burning pain, tingling,numbness, electric shock sensation typically around
ankle or at bottom of foot. - Symptoms are worse with activities like walking, standing or running,
relieved by rest,pain is usually worse at night. - Swelling around ankle and foot may be present.
Examination
- Positive compression test
- Positive tinel’s sign – tapping on the nerve posterior to the medial malleolus causes radiating pain in to the medial side of the ankle and possibly to the foot.
- Pressure within the Tarsal tunnel increases with ankle dorsiflexion and foot eversion.This may reproduce the symptoms.
- Tarsal tunnel syndrome may be present as part of heel pain triad which occurs in adults
- Heel pain triad includes Tarsal tunnel syndrome,plantar fasciitis and aquired flat foot deformity.
Diagnosis
- EMG and nerve studies
- Combination of history, examination,EMG and nerve studies can lead you to diagnosis.
- Sensory nerve conduction studies are more useful than motor nerve conduction studies.
- Always rule out radiculopathies.
- The dorsiflexion eversion test is described to be helpful in the Tarsal Tunnel syndrome.
Radiology
- Radiographs and CT may show osseous impingement or posteromedial Process fracture of the talus
- MRI may show a space occupying lesion like lipoma or ganglion cyst.
Differential Diagnosis
- Peripheral neuropathy – involves all the nerves not just the tibial nerve Sural nerve and saphenous nerve will be involved and the ankle jerk will be absent.
Treatment
- Immobilization
- Anti inflammatory medications
- Steroid injections
- Patient may have orthotic with medial posting if the patient has a valgus hind foot.
Surgical release of Tarsal tunnel if the non operative method of treatment fails after 3-6 months
- Release the fascia proximal to the flexor retinaculum
- release the flexor retinaculum
- identify the tibial nerve proximal to the tunnel and decompress the nerve and it’s 3 branches
- decompress the entire tunnel 5 cm proximal to the flexor retinaculum and distally to the deep fascia of abductor hallucis
- distal release of Baxter’s nerve is usually done if the patient has chronic plantar medial heel pain
- decompress the Baxter’s nerve by releasing the deep fascia of the Abductor hallucis remove any space occupying lessons
- Best result occur if the symptoms have occurred in less than 1 year,if the patient has a space occupying lesion with a positive physical examination and EMG findings.
- Recurrence of Tarsal tunnel syndrome is usually caused by inadequate release and repeat Tarsal tunnel release is not advisable
Nice presentation