Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
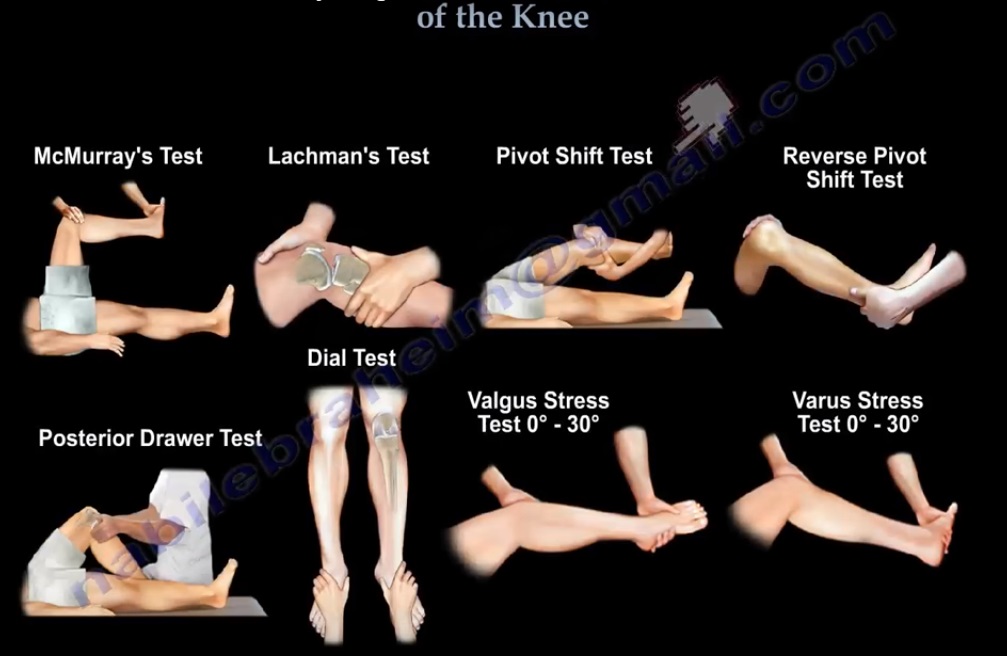
TESTS FOR EXAMINATION OF THE KNEE
MCMURRAY’S TEST is a knee examination test that elicits pain or painful click as the knee is brought from flexion to extension with either internal or external rotation. This test uses the tibia to trap the meniscus between the femoral condyle and the tibia. When performing the McMurray’s test, the patient should be lying supine with the knee flexed. The examiner then grasps the patient’s heel with one hand and places the other hand over the knee joint. To test the medial meniscus, the knee is fully flexed and the examiner then passively externally rotates the tibia and places a valgus force. The knee is then extended in order to test the medial meniscus. To test the lateral meniscus, the examiner passively internally rotates the tibia and places a varus force. The knee is then extended in order to test the lateral meniscus. A positive test is indicated by pain, clicking or popping within the joint and may signal the tear of either the medial or lateral meniscus when the knee is brought from flexion to extension.
LACHMAN’S TEST is the most sensitive examination test for ACL injury. The anterior cruciate ligament is located in front of the knee. The ACL keeps the tibia from sliding out in front of the femur and provide rotational stability to the knee. ACL tear causes anterolateral rotational instability of the knee. The patient should be lying supine and completely relaxed. Bend the knee to about 20°-30°. Stabliise the femur with one hand and with the other hand pull the tibia anteriorly and posteriorly against the femur. With an intact ACL, as the tibia is pulled forward, the examiner should feel an endpoint. If the ACL is ruptured, the ACL will be lax and the examiner will feel softer with no end point. The tibia can be pulled forward more than normal (anterior translation).
PIVOT SHIFT TEST is a specific test for ACL deficient knee (ACL injury- acute and chronic). It is pathognomic for an ACL tear and is best demonstrated in the chronic setting when there is a chronic ACL tear. The pivot shift test goes from extension (tibia subluxed) to flexion, with the tibia reduced by the iliotibial band. The patient should be lying supine and completely relaxed. With pivot shift, the knee is in the subluxed position when the knee is in full extension. The pivot shift starts with the extension of the knee and you can feel a “clunk” at 20°-30° of flexion. Hold the knee in full extension then add valgus force plus internal rotation of the tibia to increase the rotational instability of the knee. Then take the knee into flexion. You feel a palpable clunk on outside of knee as the tibia reduces. The iliotibial band will reduce the tibia and create the clunk on the outside of the knee.
REVERSE PIVOT SHIFT TEST helps to diagnose acute or chronic posterolateral instability of the knee. A significantly positive reverse pivot shift test suggests that the PCL, the LCL, the arcuate complex and the popliteofibular ligament are all torn. The test begins with patient supine with the knee in 30° of flexion. Valgus stress is then applied to the knee with an external rotation force. Bring the knee from 90° of flexion to full extension. The tibia reduces from the posterior subluxed position at about 20° of flexion. A shift and reduction of the lateral tibial plateau can be felt as it moves anteriorly from a posterior subluxed position. A “clunk” occurs as the knee is extended. This is called reverse pivot shift because the shift of the lateral tibial plateau occurs in the opposite direction of true pivot shift. If the tibia is posterolaterally subluxed, the iliotibial band will reduce the knee as the IT band transitions from a flexor to extensor of the knee.
POSTERIOR DRAWER TEST is the most accurate test for PCL injury. The posterior cruciate ligament is located in the back of the knee. PCL is the primary restraint to posterior tibial translation. PCL tear is not as common as ACL tear. The test is done with the patient in supine position and the knee is flexed to 90°. The examiner stabilised the foot. Then the examiner pushes backwards on the tibia, looking for the tibia to sag posteriorly. Observe the sag that develops due to the PCL tear. The amount of translation in relationship to the femur is observed. The test is considered positive if excessive posterior translation of the tibia is demonstrated.
DIAL TEST is to diagnose the posterolateral instability due to posterolateral corner injury with or without PCL injury. Isolated injuries of the posterolateral corners are rare and often cause instability and varus thrust. By performing the dial test, you can detect if there is an isolated or combined injury of the posterolateral corner of the knee. The test is performed with the patient in the supine or prone position with both knees in 30° and 90° of flexion. It is preferable to perform the test in the prone position. Support the thigh in position if the test is performed in supine position. An external rotation force is then applied to both feet. The amount of external rotation to both lower extremity is measured at both ankles. The testing of the injured extremity in 30° of flexion is done to determine injury to the posterolateral corner. Flexion at 90° angle will test the PCL for injury. More than 10° of external rotation compared to the other side indicates a significant injury. More than 10° of external rotation asymmetry at 30°and 90° is consistent with PLC and PCL injury(combined injury).
VALGUS STRESS TEST( 0-30°) is the test for medial collateral ligament injury. Palpate around the knee in order to check for injury to the MCL. Usually the site of tenderness and pain is above the level of knee joint and rarely below the knee joint. The best way to test the superficial part of the MCL is to place the knee in about 30° of flexion. With the MCL isolated and the knee flexed to 30°, move the knee from side to side to assess the stability of the knee. Check the opening on the medial side when valgus force is applied. Then place the knee back into 0° of full extension and test the stability of the MCL in the same way. If the MCL appears to be loose in full extension, this will signal a complete injury to the posterior capsule or cruciate ligaments in addition to injury of the MCL. Valgus force at 30° of knee flexion will test the superficial part of the MCL, which is the strongest part of MCL.
VARUS STRESS TEST(0-30°) checks for joint laxity on the outside of the knee, which usually represents an injury to the LCL. Palpate around the knee in order to check for injury to the LCL. Apply a varus force to the knee. Isolated tear of the LCL is tested at 30°of flexion. With the LCL isolated and the knee flexed to 30°, move the knee from side to side to assess for stability of the knee. Next place the knee back into 0° of full extension and test the stability of the LCL in the same way. A positive test demonstrates increased lateral joint laxity compared to the unaffected side when the varus force is applied to the knee. Varus instability at 0° and 30° of flexion indicates a combined injury of LCL and the cruciate ligaments. An isolated injury to the LCL will give you varus instability at 30° of flexion.
I love this. This is really good