Courtesy: Prof Nabil Ebraheim, University of Toledo, Ohio, USA
- Seronegative spondyloarthropathies accept approximately 10% of patients with psoriasis.
- If the spine is affected, the Human Leukocyte Antigen B27 (HLA-B27) is positive more than 50% of the time.
- The clinical presentation of psoriasis in the cervical spine could be similar to rheumatoid arthritis, but in general it is different than ankylosing spondylitis (debatable and controversial).
- Psoriatic arthritis will have negative rheumatoid factor and negative antinuclear antibody (ANA) tests.
- Psoriatic arthritis presents itself with patchy, plaques, and scales that can be red or silvery in color. It usually occurs before the arthritis and usually occurs at the elbow or the knees. It usually occurs at the extensor surface of the extremity.
- Always check the elbows! In about 20% of cases, the arthritis usually occurs before the scales and the plaques.
- This makes you wonder; why is the knee not getting better? Why is the swelling not going away?
- Psoriatic arthritis most commonly affects the hands, the feet, the spine and the sacroiliac (SI) joints.
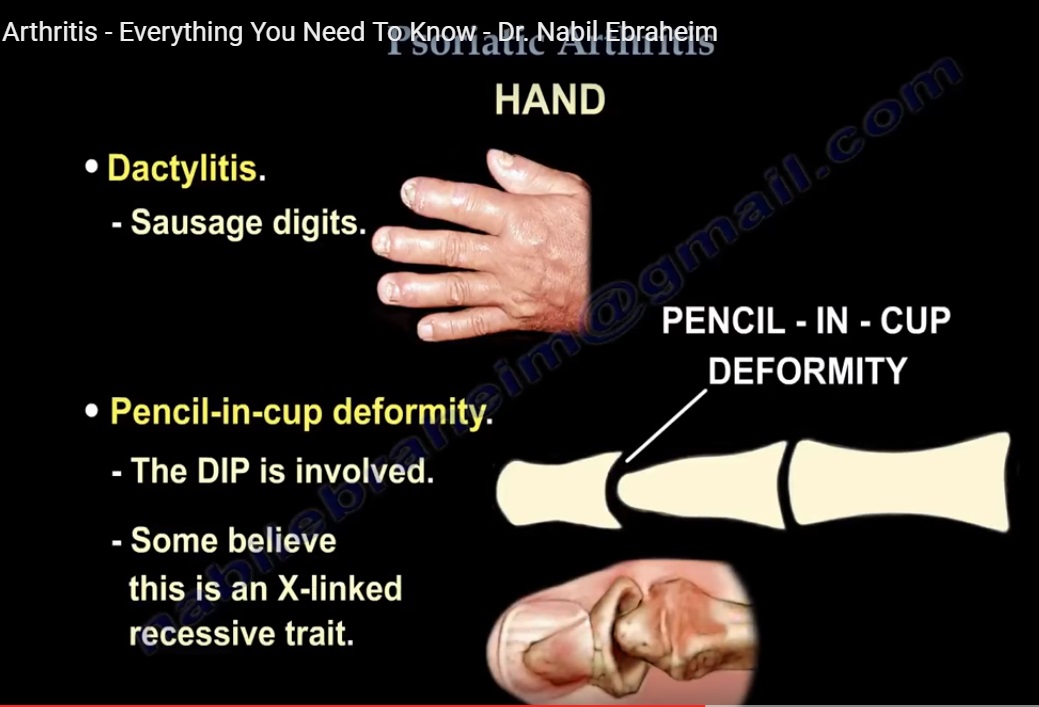
- Hand: this is very important information for clinical practice and also for the exams.
•Dactylitis: sausage digits
•Pencil-in-a-cup deformity: the DIP is involved. Some believe this is an x-linked recessive trait.
•Nail pitting: fragmentation and discoloration
•Onycholysis: lifting of the nail plate that starts distally.
•Arthritis mutilans
Also associated are
•Uveitis
•Achilles tendonitis
•Plantar fasciitis
Treatment:
- Usually medical treatment
- NSAIDs
- Methotrexate
- TNF-alpha inhibitors
- Surgery (occasionally) o
- There is a high infection with surgery
- Try to avoid skin incisions through the active psoriatic lesions (there is a high colonization with bacteria.
- Do preoperative treatment of such lesions
Leave a Reply