Courtesy: Saqib Rehman MD
Associate Professor
Director of Orthopaedic Trauma
Temple University
Philadelphia, Pennsylvania
USA
www.orthoclips.com
CHRONIC Osteomyelitis
- The term ‘osteomyelitis’ originates from the two Greek words ‘osteon’ and ‘myelos’ – bone and marrow
- The French surgeon Edouard Chassaignac was the first to introduce the term osteomyelitis in 1852
INTRODUCTION
- Chronic osteomyelitis is defined as long-standing infection of the bone characterized by persistence of microorganisms, presence of sequestrum, low-grade inflammation, and fistulae formation
- Classification
1.Duration
• Acute-4 weeks
2.Mechanism of infection
• Exogenous
• Hematogenous
3.Type of host response to the infection
• pyogenic
• nonpyogenic
Osteomyelitis Organisms and predilection for age groups
- Newborns: (younger than 4 mo): S. aureus, Enterobacter species, group A and B Streptococcus species
- Children (aged 4 mo to 4 y) : S. aureus, group A Streptococcus species, Kingella kingae, and Enterobacter species
- Children, adolescents (aged 4 y to adult): S. aureus (80%), group A Streptococcus species, H. influenzae, and Enterobacter species
- Adult: S. aureus and occasionally Enterobacter or Streptococcus species
Unusual Osteomyelitis Organisms
- Salmonella • Sickle cell anemia patients (S. aureus is still most common)
- Pseudomonas • IV drug use with AC or SC joint infection or puncture wound through rubber soled shoes
- Bartonella • HIV/AIDS patient following cat scratch or bite
- Fungal osteomyelitis • Immunosuppressed, long-term IV medications, or parenteral nutrition
- Tuberculosis • Manifestations include Potts disease
Pathophysiology
1. Host Factors
- Exogenous factors:
- Disturbances in arterial and venous circulation
- Tissue damaged by radiation
- Extensive exposure of the operation site
- Extensive soft-tissue defects
- Extensive hematomas
- Remaining hollow spaces
B.Endogenous :
- Diabetes mellitus
- Nicotine and drug use
- Nutritional deficiency
- Disturbances of liver and kidney function
- Severe infections with immunosuppression
2.ENVIRONMENTAL FACTORS
- Skin preparation
- Operating room environment
- Prophylactic antibiotics
- Tissue handling
- Orthopedic implants
3.BACTERIOLOGIC FACTORS
- Sequestrum : devitalized avascular segment of bone, surrounded, by pus /infected granulation tissue and is more dense than surrounding bone
- Involucrum :-derived from the word “volvere” i.e. to wrap .It is the result of reactive new bone formed by periosteal reaction , in an attempt to wall off the infection by forming a thick tense wall
- Cloacae -single or multiple openings in involucrum and are caused by rupture of periosteum due to pus under tension .
PRESENTATION
• Symptoms-pain,fever,(m.c in acute osteomyelitis)
• fever, tachycardia, and hypotension suggest sepsis
• Inspection-erythema, tenderness, edema
• draining sinus tract-common in chronic osteomyelitis
• limp and/or pain inhibition with weight-bearing or motion may be present
LABORATORY ANALYSIS
- Leukocyte Count (WBC),ESR,CRP
- Blood culture
- Sinus Tract Cultures
- Culture Of Bone–gold-standard
- Serum procalcitonin-increased in infection and trauma
- PCR- mycoplasma pnuemonia, brucella, bartonella
- Bone biopsy AND Histopathological examination
IMAGING
- Radiographs: bone lucency, sclerotic rim, osteopenia, periosteal reaction, and lysis around hardware
- USG
- CT SCAN
- MRI- RIM SIGN AND PENUMBRA SIGN
- SINOGRAPHY
- 3 phase bone scintigraphy
- PET scan
- Nuclear medicine-TECHNETIUM BONE SCAN, GALLIUM SCAN, Indium-111–labeled leukocyte scans
Diagnostic criteria-MORREY AND PETERSON
- Definite-The pathogen is isolated from bone /tissue or there is histologic evidence of osteomyelitis
- Propable-blood culture positive in setting of clinical and radiographic features of osteomyelitis
- Likely-typical clinical findings and definitive radiographic evidences are present with response to antibiotic therapy
Chronic osteomyelitis
- Hallmark : infected dead bone within a compromised soft-tissue envelope
- Persisting , productive form of bone inflammation is characterized by chronic purulent fistulous discharge- which originates from sequestra
- Negative charge on surface of devitalized bone promotes organism adherence and subsequent glycocalyx formation thereby preventing access to phagocytes & microbials.
- Bacteria enter the interior of the cell eluding host defense. Dead & dying osteoblast release viable S. Aureus causing persistence of infection & its flare up.
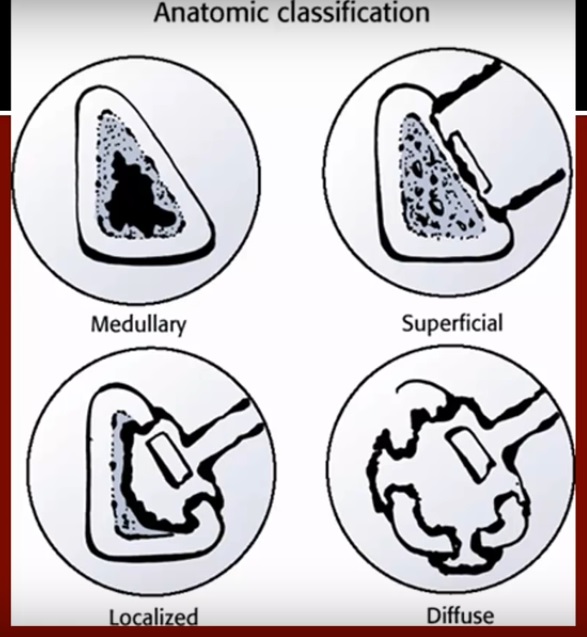
Classification of chronic osteomyelitis
Anatomic Location
- Stage 1 • Medullary
- Stage 2 • Superficial
- Stage 3 • Localized
- Stage 4 • Diffuse
Host type
- Type A • Normal
- Type BL • Locally compromised
- Type BS • Systemically compromised
- Type C • Treatment is worse to the patient than infection
Treatment
Multifaceted approach
Surgery for chronic osteomyelitis consists of
1. sequestrectomy
2. Saucerisation-The limits of debridement have classically been determined by the paprika sign’, which is punctuate cortical or cancellous bleeding.
Soft-tissue and dead-space management
- Bone grafting with primary and secondary closure
- PMMA beads as temporary filler
- Local muscle flaps and skin grafting +/- bone grafting
- Microvascular transfer of muscle
- Myocutaneous,osteocutaneous flaps
- Bone transport –ilizarov ring fixator- radical surgery
- Antibiotics management:6-week course of intravenous antibiotics(total duration of antibiotic therapy is suggested as 4-8 weeks)
- modified Lautenbach method-Closed suction drains
OPEN BONE GRAFTING
• classical Papineau technique
• STAGE I: DEBRIDEMENT AND STABILIZATION
• STAGE II: GRAFTING
• STAGE III: WOUND COVERAGE
Two stage Belfast technique
• radical debridement followed by immediate provision of soft tissue cover. In addition, and when indicated, delayed autogenous bone grafting was also performed at the second stage
Masquelet technique or the induced membrane technique
• This two-stage technique relies upon filling the segmental defect with a solid block of PMMA, which over 6-8 weeks becomes surrounded by a highly cellular bio-membrane.
• At reoperation the membrane is incised, the cement is removed and replaced with bone graft
POLYMETHYLMETHACRYLATE ANTIBIOTIC BEAD CHAINS
- Deliver levels of antibiotics locally in concentrations that exceed the minimal inhibitory concentrations
BIODEGRADABLE ANTIBIOTIC DELIVERY SYSTEMS
- Bioactive glass
DISTRACTION OSTEOGENESIS
ADJUNCTIVE THERAPIES-
- Hyperbaric oxygen therapy
- Growth factors, such as bone morphogenic proteins (BMPs) and even platelet-rich plasma (PRP)
- Pulsed electromagnetic fields [PEMF] and ultrasound
Amputation-reserved only for those extreme cases of chronic osteomyelitis
Treatment based on CIERNY –MADER classification
• Type 1- drainage and curettage of dead space with simple closure and antibiotics administration
• Type 2- curettage and treatment of dead space with soft tissue envolope
• Type 3-complex drainage and curettage of dead space with removal of bone and complex closure.stabilisation+/-
• Type 4- type 3 management+ skeletal stabilisation (instability-large bone portion removal)
I like this page.