Advances in the Diagnosis of the Forearm Interosseous Ligament (IOL) Rupture
 Amir R. Kachooei, MD, Orthopedic Hand and Elbow Surgeon
Amir R. Kachooei, MD, Orthopedic Hand and Elbow Surgeon
Mashhad University of Medical Sciences, Mashhad, Iran
Massachusetts General Hospital, Harvard Medical School, Boston, USA
Kachooei AR, Rivlin M, Shojaie B, van Dijk CN, Mudgal C. Intraoperative Technique for Evaluation of the Interosseous Ligament of the Forearm. J Hand Surg Am. 2015;40(12):2372-6.e1.
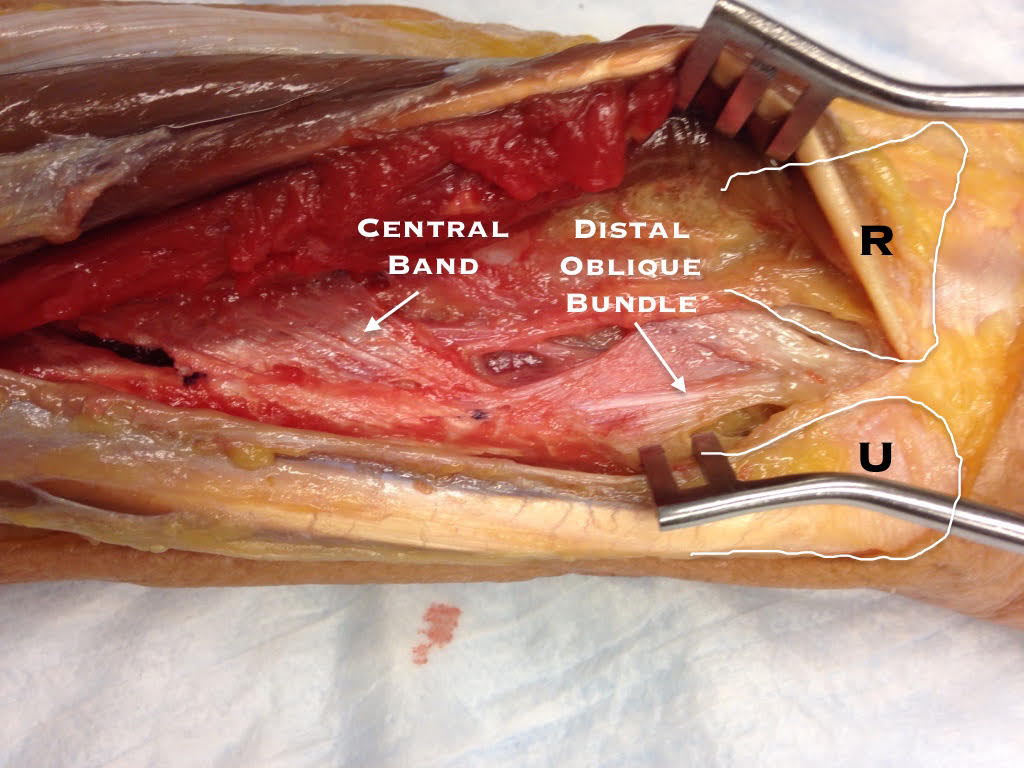
Forearm interosseous ligament (IOL) disruption can be difficult to diagnosis and is often recognized late[Figure 1].
 Current methods to assess the integrity of the IOL are MRI and ultrasonography; however, it is cumbersome to perform imaging in an emergent event. The ability to diagnose clinically and intra-operatively will help us avoid missing the diagnosis and undertake an optimal strategy at the index operation. Two techniques of examination were introduced to help diagnose the IOL rupture intra-operatively. Smith et al described the “radius pull test” in which longitudinal traction on radius after resecting the radial head allows radius to move proximally whenthe IOL is cut(1). Recently, Soubeyrand et al described the “radius joystick” test and showed that the lateral displacement of proximal radius remarkably increased after IOL rupture while the forearm was in full pronation (2).
Current methods to assess the integrity of the IOL are MRI and ultrasonography; however, it is cumbersome to perform imaging in an emergent event. The ability to diagnose clinically and intra-operatively will help us avoid missing the diagnosis and undertake an optimal strategy at the index operation. Two techniques of examination were introduced to help diagnose the IOL rupture intra-operatively. Smith et al described the “radius pull test” in which longitudinal traction on radius after resecting the radial head allows radius to move proximally whenthe IOL is cut(1). Recently, Soubeyrand et al described the “radius joystick” test and showed that the lateral displacement of proximal radius remarkably increased after IOL rupture while the forearm was in full pronation (2).
Considering the above mentioned examination techniques, we aimed to test the inter- and intra-observer reliability of the diagnosis of the IOL rupture using both techniques. This may show how much we can rely on clinical judgment in deciding whether radial head resection without replacement is contraindicated. The results of our study showed fair inter-observer and moderate intra-observer reliability for diagnosis of the IOL injury using clinical examination. Diagnostic performance characteristics of both tests together (Specificity, sensitivity, positive and negative predictive values, and accuracy) were all around 70% in both rounds of examination. The positive and negative likelihood ratio showed that the tests are ‘sometimes useful’. The second round of examination showed small improvement in results but the difference was not yet remarkable. Most of the examiners expressed low level of confidence in terms of deciding whether IOL is ruptured or not(3).
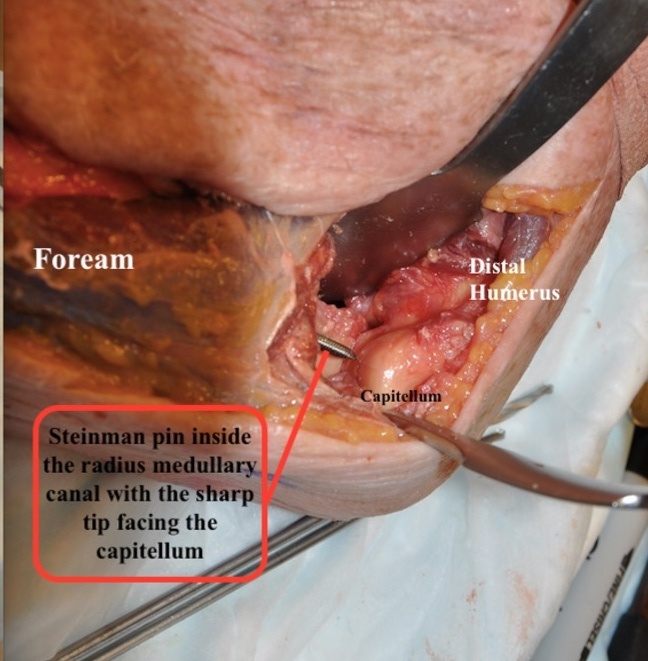
Because these tests showed low level of reliability, we decided to determine the best position to test the IOL[Figure 2]
 In contrast to the “joystick radius test” that was explained in full pronation as the most stable position (the test was considered negative if no mobilization occurred with the pull), our results showed that the highest stiffness is in forearm supination with the least amount of displacement when the IOL is intact. The amount of displacement in pronation was approximately the same as neural position showing that the IOL is relaxed with pronation of the forearm(4). This position has also been confirmed in other biomechanical studies showing highest amount of stiffness in supination.
In contrast to the “joystick radius test” that was explained in full pronation as the most stable position (the test was considered negative if no mobilization occurred with the pull), our results showed that the highest stiffness is in forearm supination with the least amount of displacement when the IOL is intact. The amount of displacement in pronation was approximately the same as neural position showing that the IOL is relaxed with pronation of the forearm(4). This position has also been confirmed in other biomechanical studies showing highest amount of stiffness in supination.
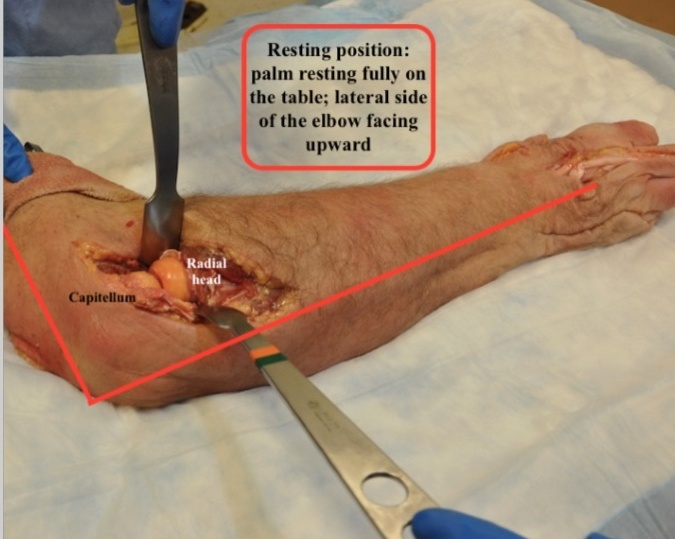
We then studied the amount of lateral displacement after radial head resection to find a cut-off for the diagnosis of the IOL rupture[Figure 3].
 Accounting for the highest sensitivity in the diagnosis of IOL disruption, the cutoff value of 5.5 mm lateral displacement in elbow extension-supination had 100% sensitivity and 90% specificity. In elbow flexion-supination, the cutoff value of 9 mm had 100% sensitivity and 90% specificity in the diagnosis of IOL disruption(4). This maneuver was shown to be reliable and accurate in cadavers with complete IOL disruption. However, its efficacy in partial injuries merits future studies on a larger number of cadavers.
Accounting for the highest sensitivity in the diagnosis of IOL disruption, the cutoff value of 5.5 mm lateral displacement in elbow extension-supination had 100% sensitivity and 90% specificity. In elbow flexion-supination, the cutoff value of 9 mm had 100% sensitivity and 90% specificity in the diagnosis of IOL disruption(4). This maneuver was shown to be reliable and accurate in cadavers with complete IOL disruption. However, its efficacy in partial injuries merits future studies on a larger number of cadavers.
References:
- Smith AM, Urbanosky LR, Castle JA, Rushing JT, Ruch DS. Radius pull test: predictor of longitudinal forearm instability. J Bone Joint Surg Am. 2002;84-A(11):1970-6.
- Soubeyrand M, Ciais G, Wassermann V, Kalouche I, Biau D, Dumontier C, et al. The intra-operative radius joystick test to diagnose complete disruption of the interosseous membrane. J Bone Joint Surg Br. 2011;93(10):1389-94.
- Kachooei AR, Rivlin M, Wu F, Faghfouri A, Eberlin KR, Ring D. Intraoperative Physical Examination for Diagnosis of Interosseous Ligament Rupture-Cadaveric Study. J Hand Surg Am. 2015;40(9):1785-90.e1.
- Kachooei AR, Rivlin M, Shojaie B, van Dijk CN, Mudgal C. Intraoperative Technique for Evaluation of the Interosseous Ligament of the Forearm. J Hand Surg Am. 2015;40(12):2372-6.e1.
Leave a Reply